
The Septal R Wave in V1 and V2: Anatomy, Physiology, and Clinical Relevance
Oct 30, 2025One of the subtle but critical features on the ECG is the septal R wave in the right precordial leads (V1 and V2). This small deflection often gets overlooked, but it reflects a very specific sequence of cardiac activation and provides important insight into normal conduction and anatomy. Understanding the septal R wave requires us to revisit the anatomy of the interventricular septum and the physiology of ventricular depolarization.
Related Topics:
The Anatomy of the Interventricular Septum
The interventricular septum isn’t uniform—it has two distinct parts:
-
Muscular septum – the thick lower portion that makes up the majority of the septum.
-
Membranous septum – the thinner upper portion near the atrioventricular junction.
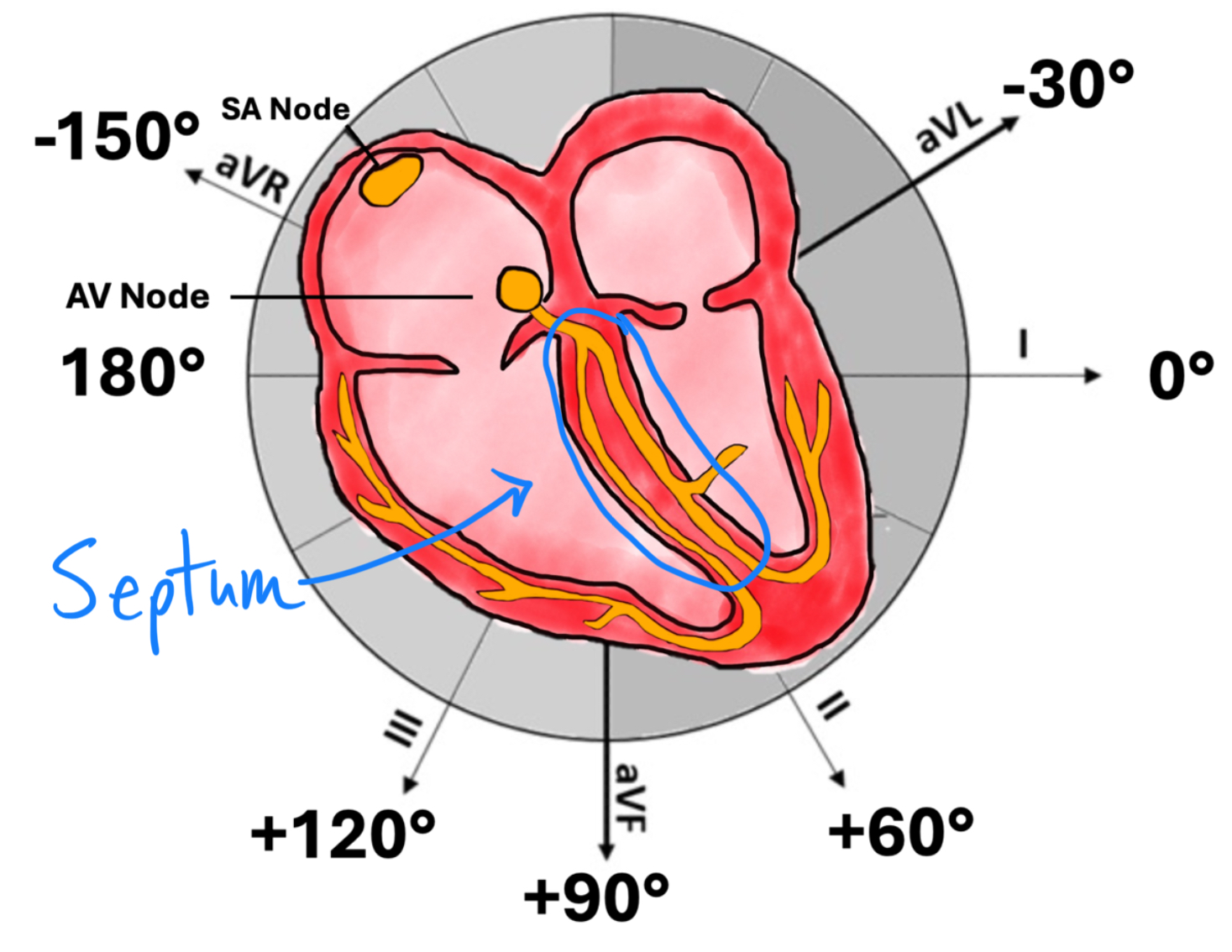
Embedded within the septum is the conduction system:
-
The bundle of His courses through the membranous septum before dividing.
-
The left bundle branch splits into anterior and posterior fascicles that spread across the left ventricle.
-
The right bundle branch runs down the right side of the septum.
This anatomic arrangement explains why septal depolarization begins left to right, producing the small R waves in V1–V2.
Physiology of Septal Activation
Stepwise Depolarization:
-
Impulse from the His bundle enters the left bundle branch slightly before the right.
-
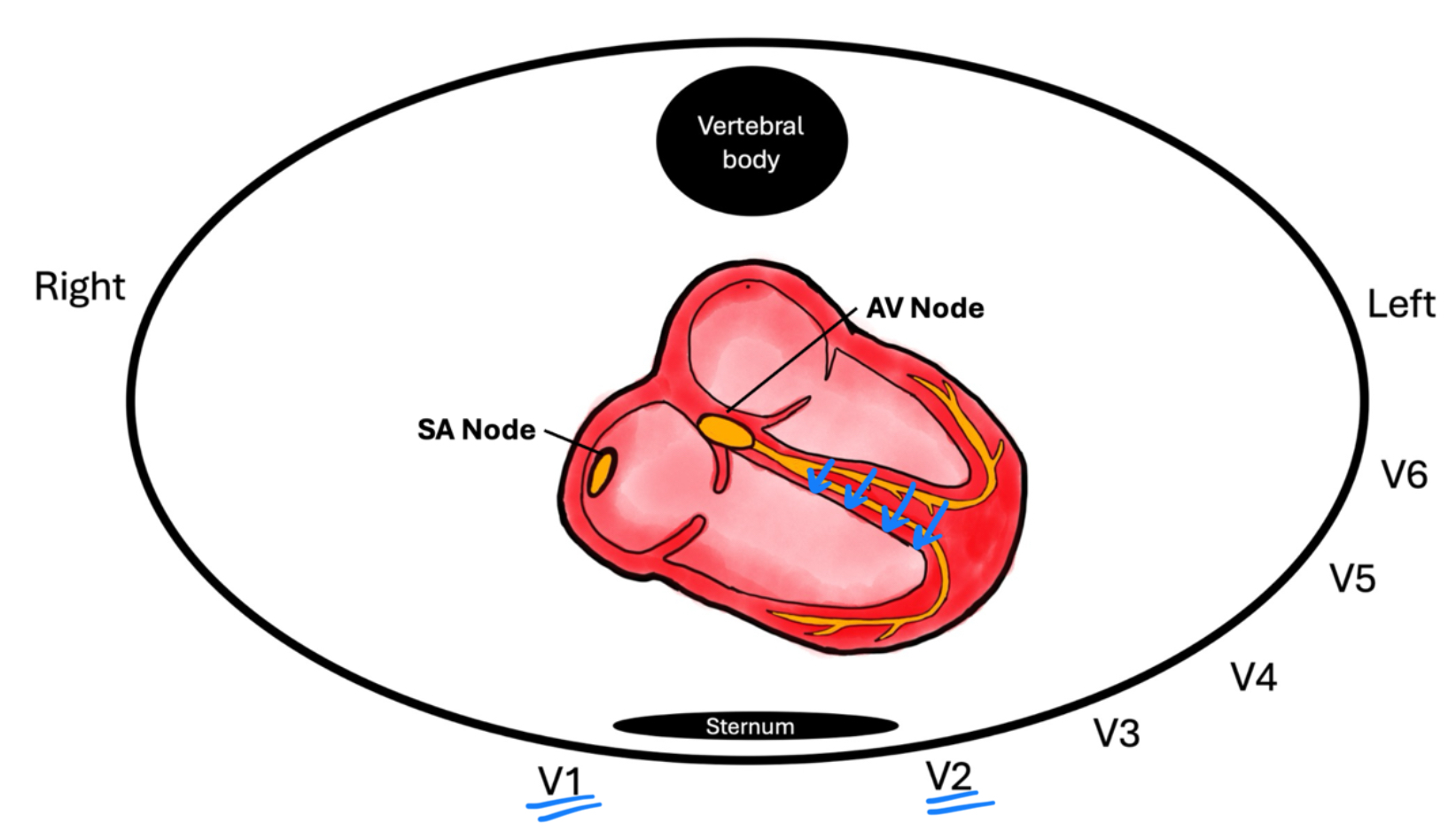
Septal depolarization begins left-to-right, activating the mid-septum toward the right ventricle.
-
This left-to-right vector is captured in the right precordial leads (V1–V2) as a small positive deflection: the septal R wave.
-
Almost immediately after, the large mass of the left ventricle depolarizes, producing a dominant S wave in V1–V2.
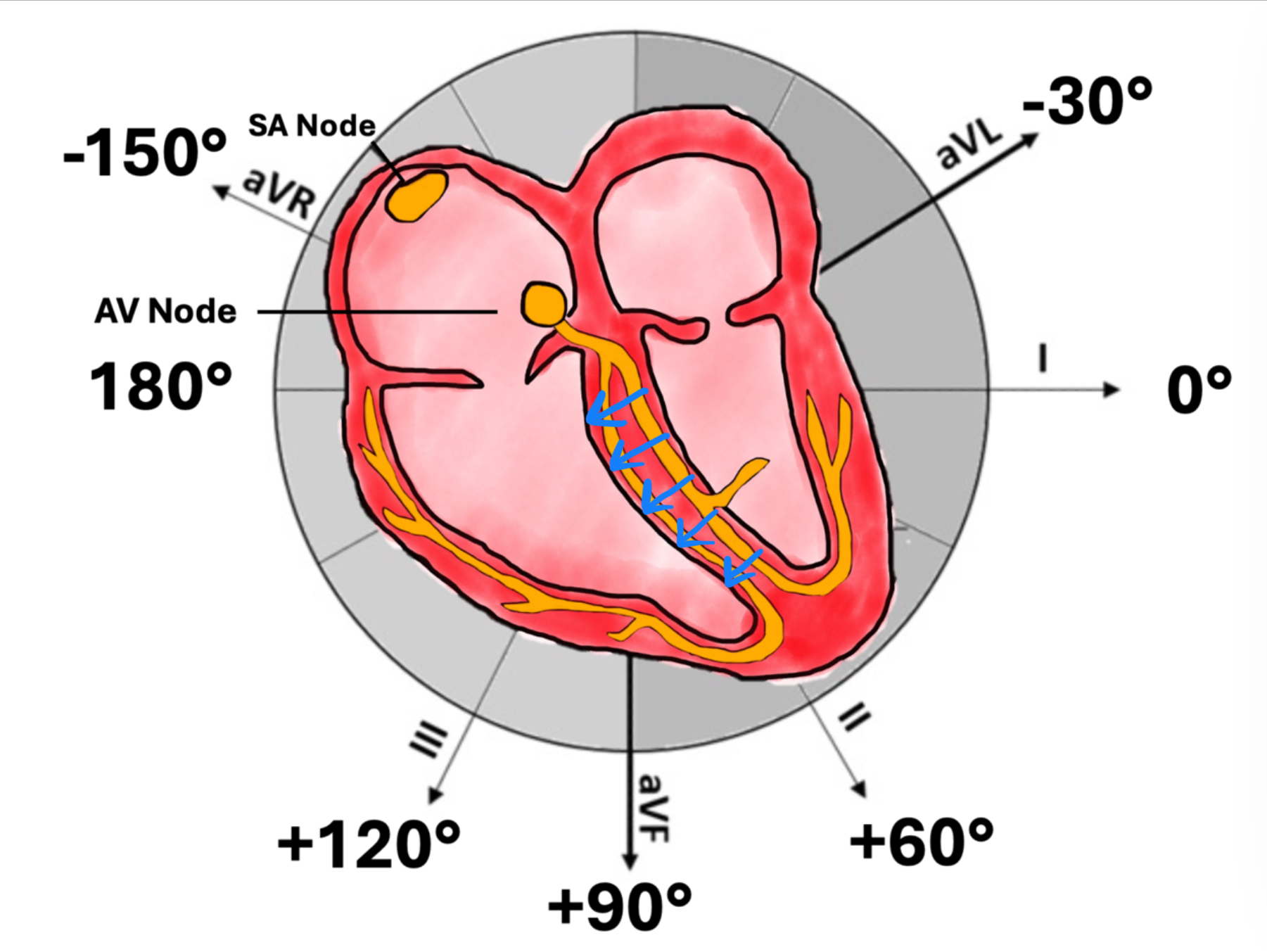

Key Concept:
The septal R wave is not about right ventricular activation—it’s about the earliest left-to-right depolarization of the interventricular septum.
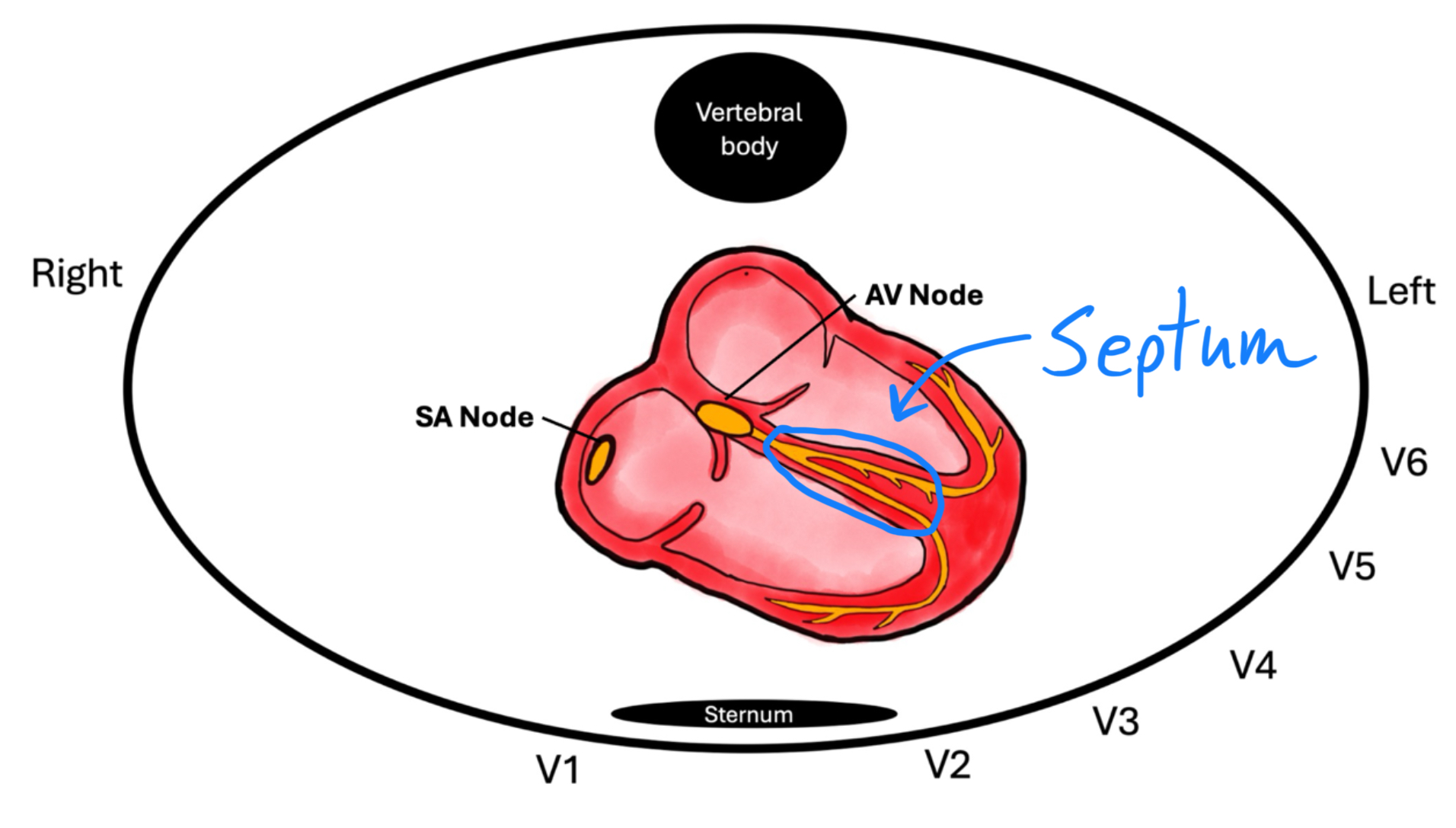
ECG Appearance of the Septal R Wave
-
Leads: Seen in V1 and V2.
-
Size: Small, typically <3 mm in amplitude.
-
Duration: Narrow, as it reflects a brisk conduction across the septum.
-
Morphology: Appears as an rS complex (small r followed by deep S).
When the Septal R Wave is Abnormal
Loss or alteration of the septal R wave can be an important clinical clue:
-
Left Bundle Branch Block (LBBB)
-
The septum depolarizes right-to-left instead of left-to-right.
-
Result: Septal R wave disappears in V1–V2 (deep QS complex).
-
-
Anterior Myocardial Infarction
-
Infarction of the septum (often LAD territory) can eliminate the septal vector.
-
Result: Pathologic Q waves or absence of septal R waves in V1–V2.
-
-
Ventricular Pre-excitation (WPW)
-
Accessory pathway conduction may bypass the normal His-Purkinje sequence.
-
Septal activation becomes abnormal, altering or abolishing the expected septal R.
-
-
Right Ventricular Hypertrophy or Conduction Delay
-
May exaggerate or distort the rS pattern in V1–V2.
-
Enjoy this style of lecture and looking to learn more? Click below to learn more about how you can join my complete ECG course.
ECG With Reid Academy
Accredited by the AMA, AAPA, ANCC, ACPE & more.
