
P-Wave Morphology in Premature Atrial Contractions
Nov 30, 2025Premature atrial contractions (PACs) are often dismissed as benign timing errors, but their diagnostic value lies in the details—especially the P-wave morphology and how that ectopic atrial impulse navigates the conduction system. For clinicians reading ECGs at a high level, PACs offer a window into atrial anatomy, conduction physiology, and even latent nodal or His–Purkinje disease.
1. Why the P Wave Changes in PACs
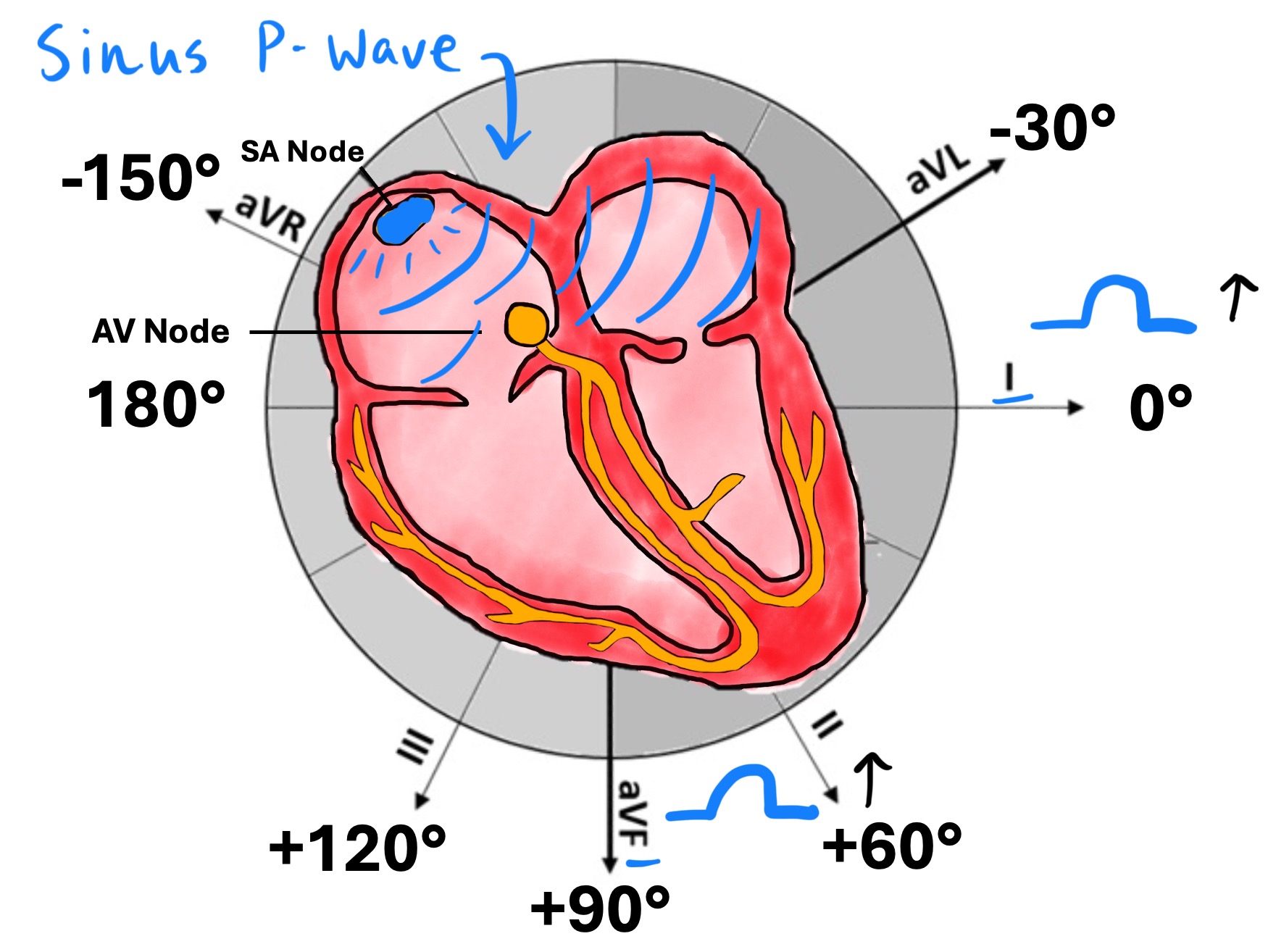
A PAC originates from an atrial focus outside the sinus node, meaning the atria depolarize along a different pathway than the standard superior-to-inferior, right-to-left sinus vector.
Because the source of depolarization shifts, several predictable changes occur:
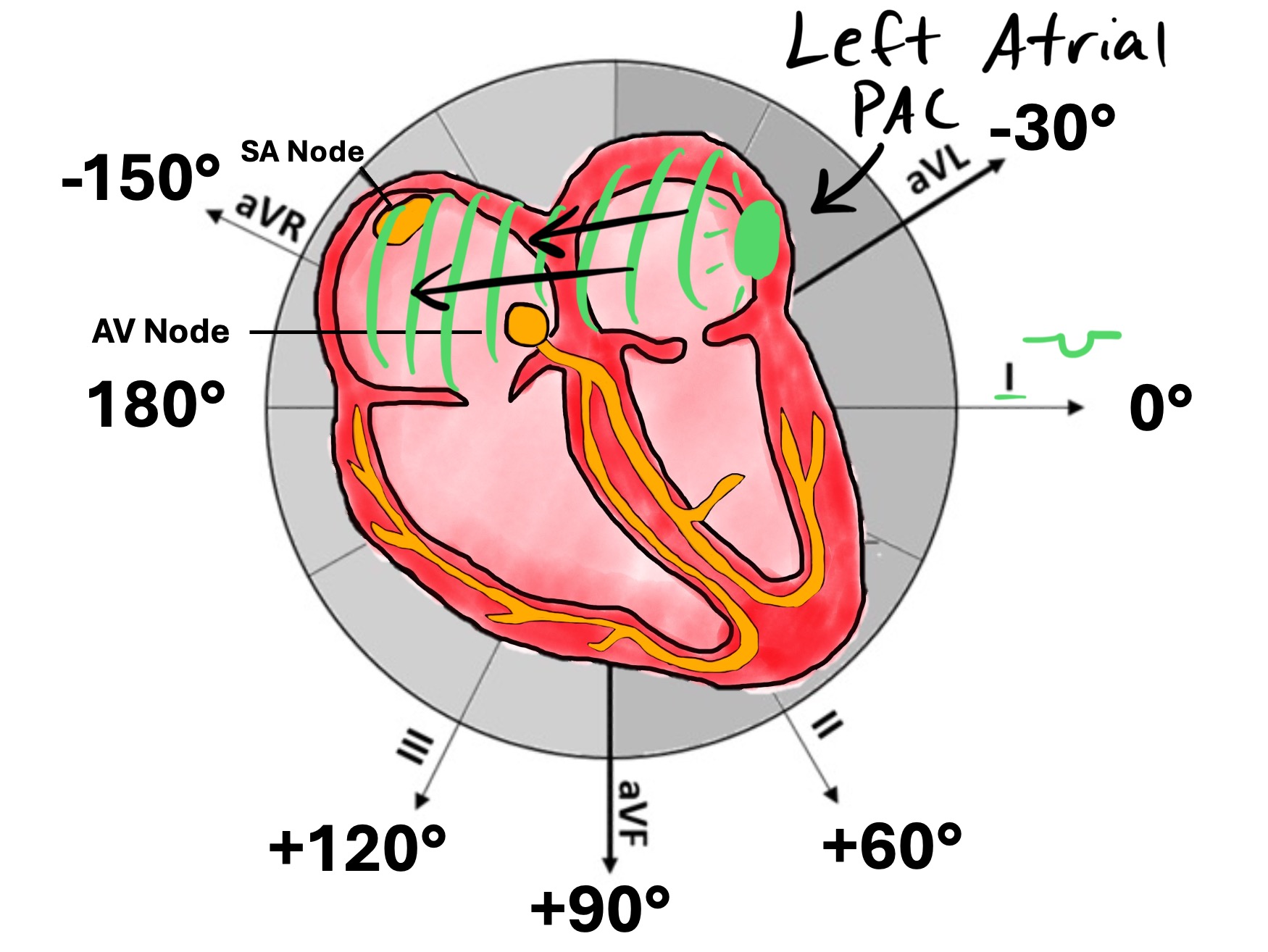
A. Abnormal P-wave axis
-
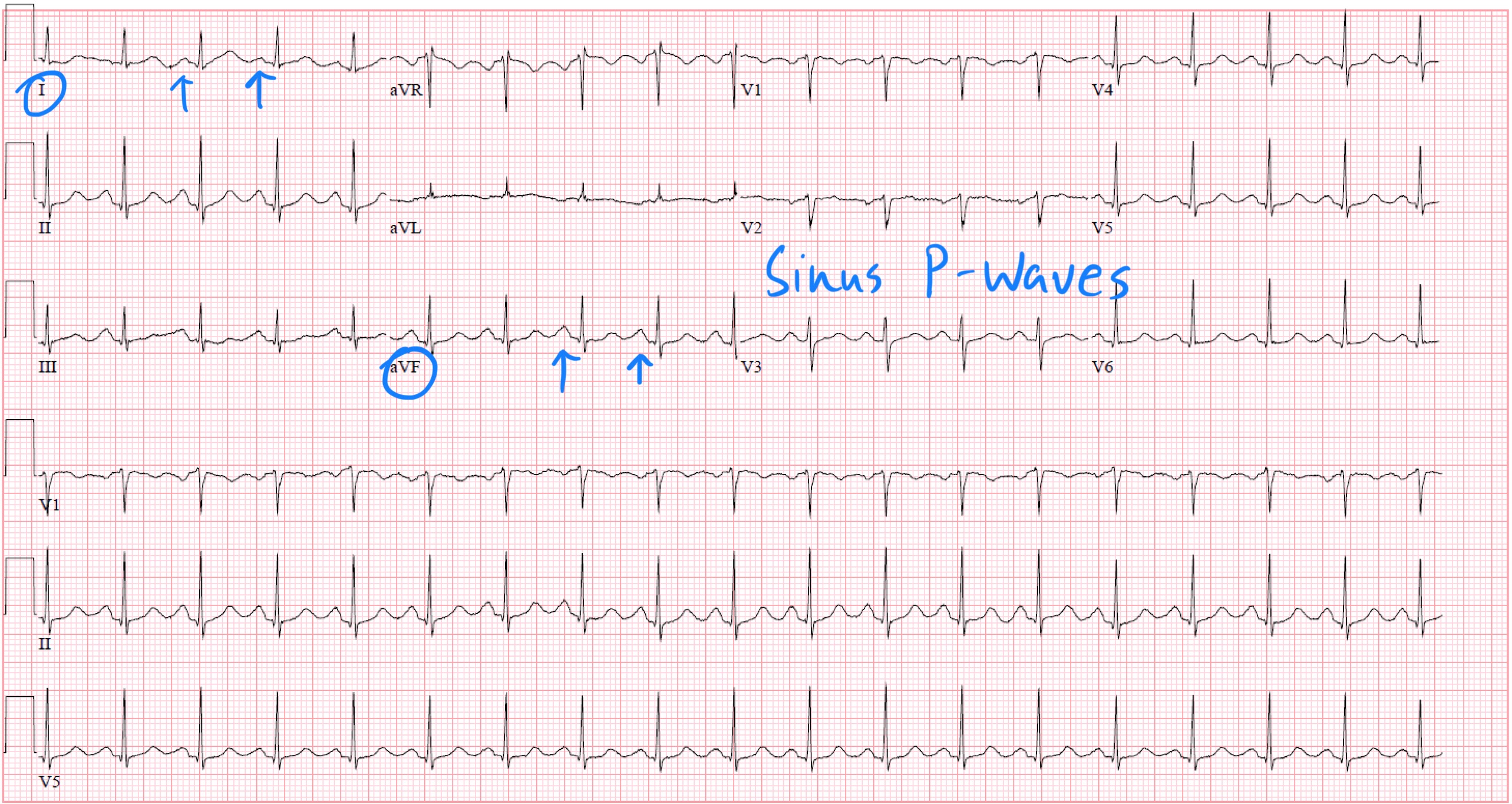
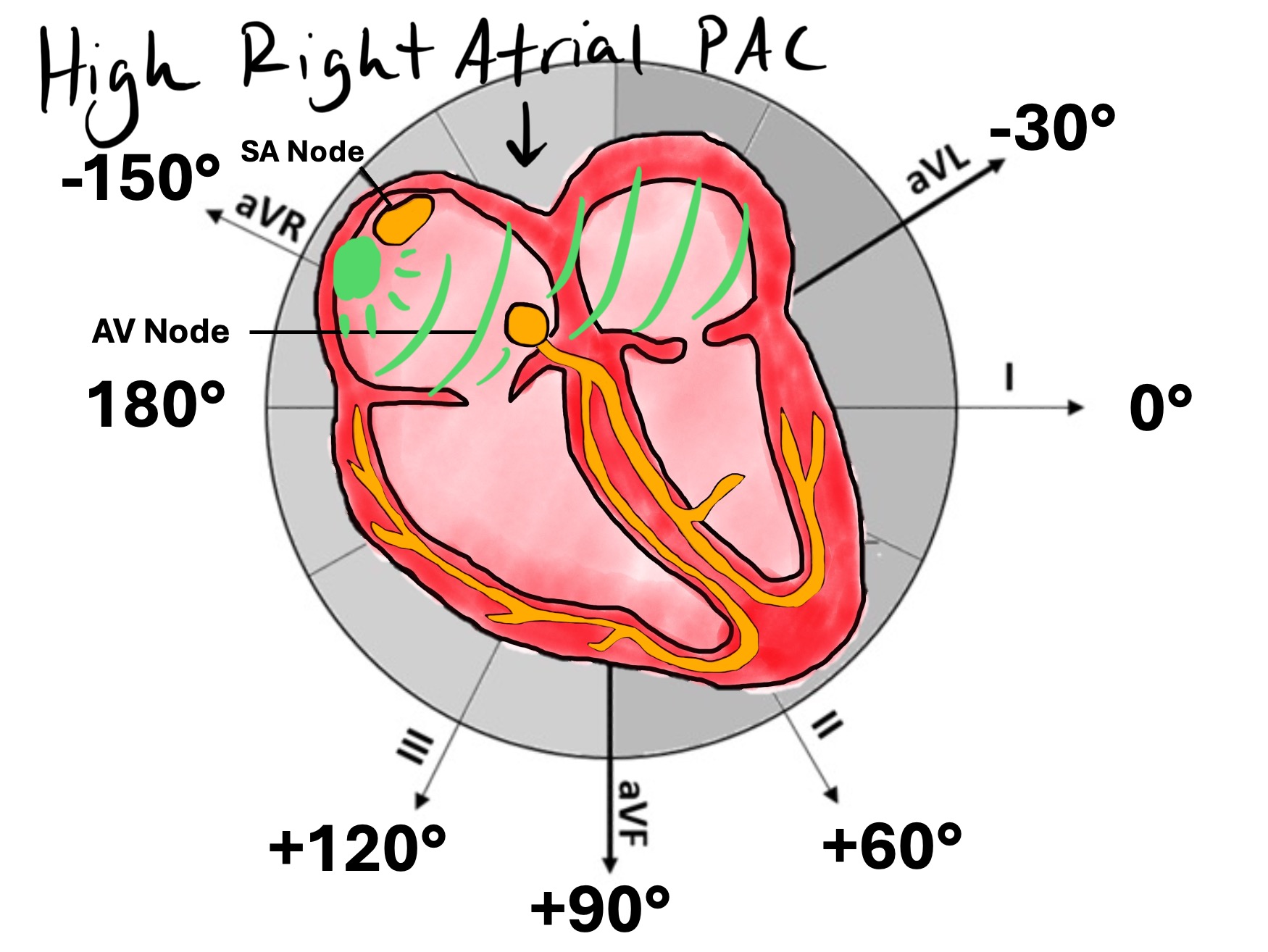
High-right atrial PAC → P waves may resemble sinus P waves but are often slightly earlier, narrower, or subtly different in axis.
-
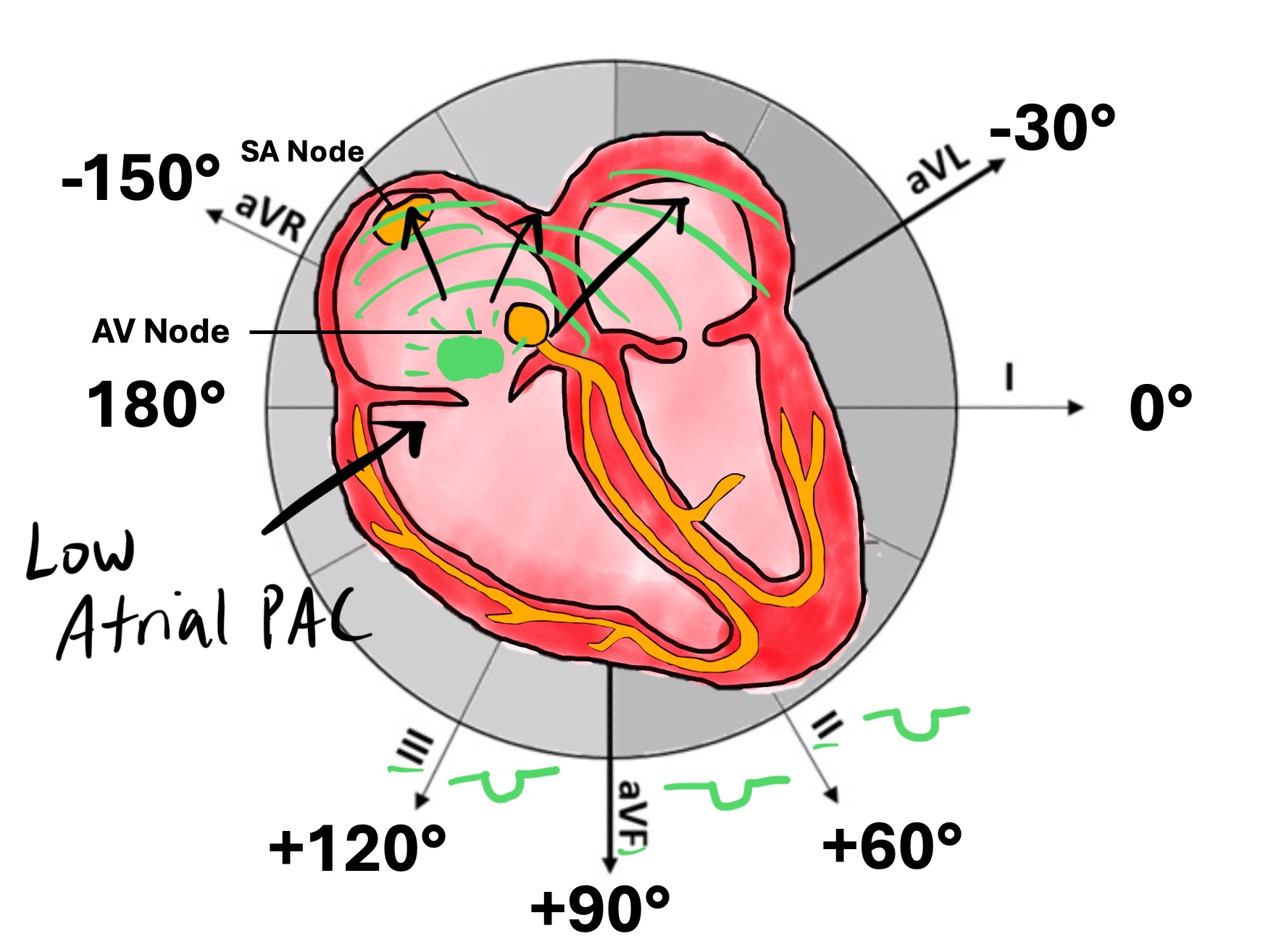
Low-atrial PAC → Retrograde activation of the atria creates inverted P waves in II, III, aVF.
-
Left-atrial PAC → P waves will become negative in Lead I.
The key is not “abnormal vs. normal” but “different from the patient’s sinus morphology.”
B. Altered P-wave timing
PACs occur early, which means:
-
They may encroach on the preceding T wave.
-
The ectopic P may be partially hidden or distort the T wave.
-
Very early PACs may conduct aberrantly (Ashman phenomenon).
This early timing is the physiologic trigger for downstream conduction changes.
2. How PACs Alter Conduction Through the AV Node
The AV node is rate-dependent and highly sensitive to timing. When a PAC arrives:
-
If the AV node has recovered → It conducts normally with a normal PR interval.
-
If partially refractory → It conducts with prolonged PR due to slowing within the node.
-
If significantly refractory → It may produce non-conducted PACs (a P wave not followed by a QRS). Read more about this here.
This is why non-conducted PACs are one of the most commonly misdiagnosed rhythms—you must identify the early, abnormal P wave buried in the preceding T wave.
3. How PACs Interact With the His–Purkinje System
A PAC often reaches the ventricles at a time when one bundle branch is refractory and the other is recovered. This produces:
-
Functional bundle branch block (aberrancy)
-
Typically, RBBB pattern due to longer right-bundle refractoriness.
-
This is the mechanism behind the Ashman phenomenon when long-short cycles occur.
- Read more about Functional RBBB here.
-
The morphology of the QRS after a PAC can therefore reveal:
-
Hidden His–Purkinje disease
-
Unmasked rate-dependent conduction delay
-
Whether the ectopic impulse was early enough to encounter differential refractoriness
Enjoy this style of lecture and looking to learn more? Click below to learn more about how you can join my complete ECG course.
ECG With Reid Academy
Accredited by the AMA, AAPA, ANCC, ACPE & more.
