
Blocked PACs: ECG Findings and Underlying Pathophysiology
Sep 11, 2025Premature atrial contractions (PACs) are a common finding on ECG and are usually benign. But sometimes a PAC arrives at the AV node when it is still refractory, preventing ventricular conduction. The result is a blocked PAC—an event that can easily be mistaken for sinus node dysfunction or pathological AV block.
Understanding the ECG pattern and the AV nodal physiology behind blocked PACs is crucial to avoid misdiagnosis and to correctly interpret pauses on the ECG.
The Physiology of a Blocked PAC
-
A PAC originates in the atria outside the sinus node.
-
It depolarizes the atria (producing a P wave on the ECG), but the impulse arrives at the AV node prematurely.
-
Because the AV node has a relatively long refractory period (due to calcium channel–mediated slow conduction and decremental properties), it may still be recovering from the previous beat.
-
The premature atrial impulse fails to conduct to the ventricles, so no QRS complex follows.
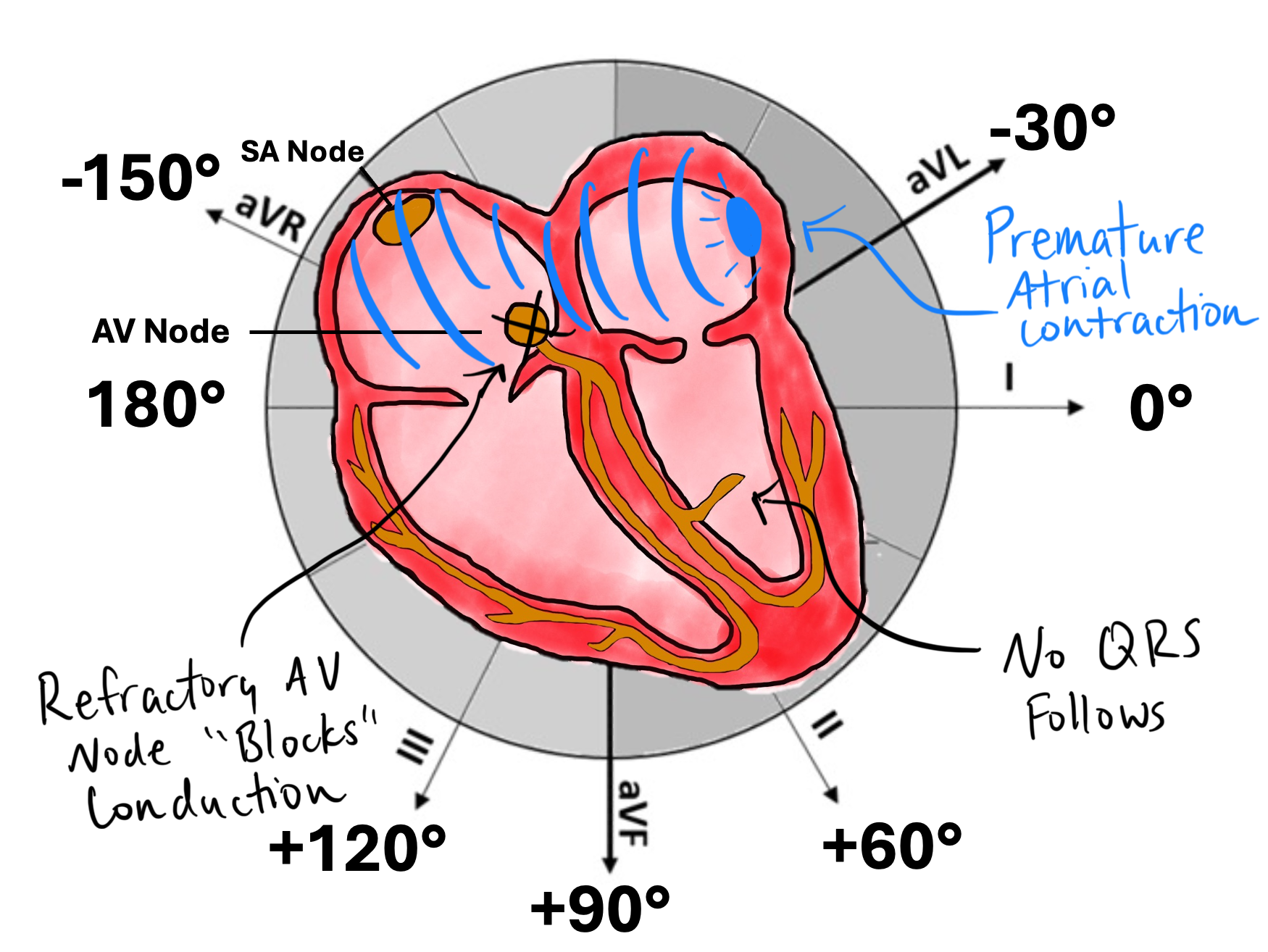
This is the mechanism of a blocked PAC: atrial activity occurs, but the ventricles remain silent.
ECG Findings of a Blocked PAC


-
Early, abnormal P wave
-
Appears sooner than expected in the sinus cycle.
-
Has a different morphology than the sinus P wave (since its origin is ectopic).
-
-
No QRS complex follows
-
The P wave is “non-conducted” because the AV node is refractory.
-
This produces a pause in the rhythm.
-
-
Compensatory pause
-
The timing of the pause depends on whether the PAC resets the sinus node:
-
If the PAC resets the sinus node, the next sinus P wave is delayed.
-
If it does not reset the sinus node, the pause may appear as a multiple of the basic sinus cycle length.
-
-
-
Key clue: a “hidden” P wave
-
Sometimes the premature P wave is subtle, buried in the T wave of the preceding beat.
-
This can make a blocked PAC appear as if there was simply a dropped QRS or a sinus pause.
-
Differentiating a Blocked PAC from AV Block or Sinus Pause
-
Sinus pause/arrest: no premature P wave is seen; the sinus node simply fails to fire.
-
Mobitz II AV block: P waves are regular and “on time,” but some fail to conduct.
-
Blocked PAC: an early, abnormal P wave precedes the pause, often hidden in the T wave.
Pearl: If you see a sudden pause in rhythm, look closely at the T waves—there may be a premature P wave hiding there.
Clinical Significance
-
Blocked PACs are benign in most cases and require no treatment.
-
They are commonly seen in patients with heightened atrial irritability:
-
Stress, caffeine, stimulants
-
Structural heart disease
-
Electrolyte disturbances
-
-
Misinterpreting blocked PACs as sinus node dysfunction or Mobitz II AV block may lead to unnecessary interventions, including pacemaker placement.
Take-Home Points
-
Blocked PACs occur when a premature atrial impulse reaches the AV node while it is refractory, preventing ventricular conduction.
-
On ECG, look for an early abnormal P wave without a QRS, often hidden in the T wave.
-
They can mimic sinus pauses or AV block, but recognizing the premature P wave is the key.
-
Usually benign, but accurate recognition avoids inappropriate management.
Enjoy this style of lecture and looking to learn more? Click below to learn more about how you can join my complete ECG course.
ECG With Reid Academy
Accredited by the AMA, AAPA, ANCC, ACPE & more.
