
Understanding AV Nodal Reentry Tachycardia (AVNRT): Mechanism, Initiation, and Treatment Rationale
Jun 05, 2025AV Nodal Reentry Tachycardia (AVNRT) is one of the most common types of paroxysmal supraventricular tachycardia (PSVT), frequently encountered in the emergency department and electrophysiology lab. It arises not from an ectopic focus, but from a reentrant circuit within or around the AV node, exploiting the physiology of dual AV nodal pathways. To understand both how AVNRT initiates and why certain treatments work, we must explore the anatomy and electrophysiology of this unique reentrant rhythm.
Dual AV Nodal Pathways: The Substrate for Reentry
Most individuals have functionally dual pathways within the AV node:
-
Slow pathway: Conducts impulses slowly but has a shorter refractory period
-
Fast pathway: Conducts impulses rapidly but has a longer refractory period
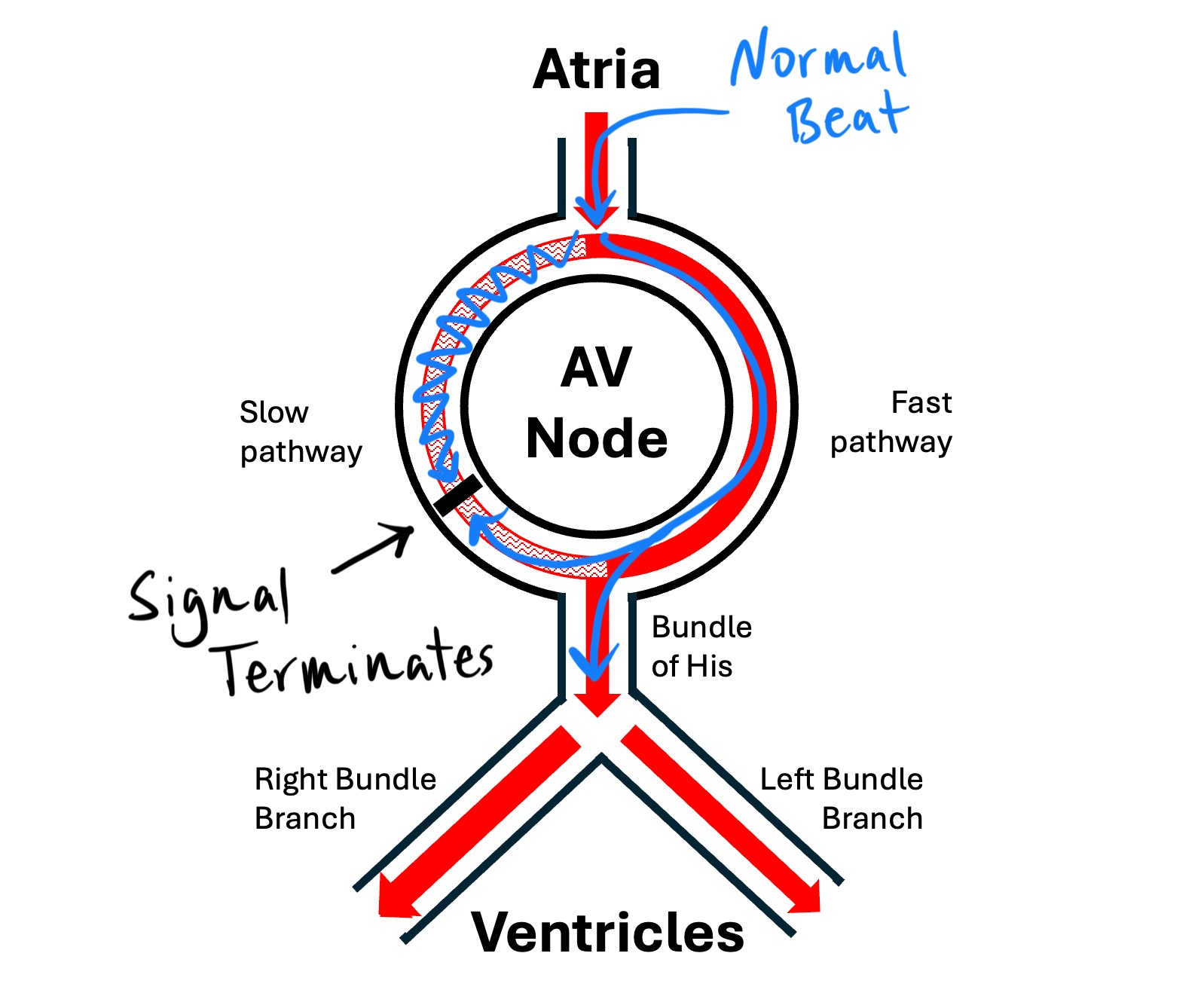
Under normal sinus rhythm, conduction typically proceeds down the fast pathway, as it's the quickest route to the ventricles.
The AVNRT Mechanism: Setting Up the Loop
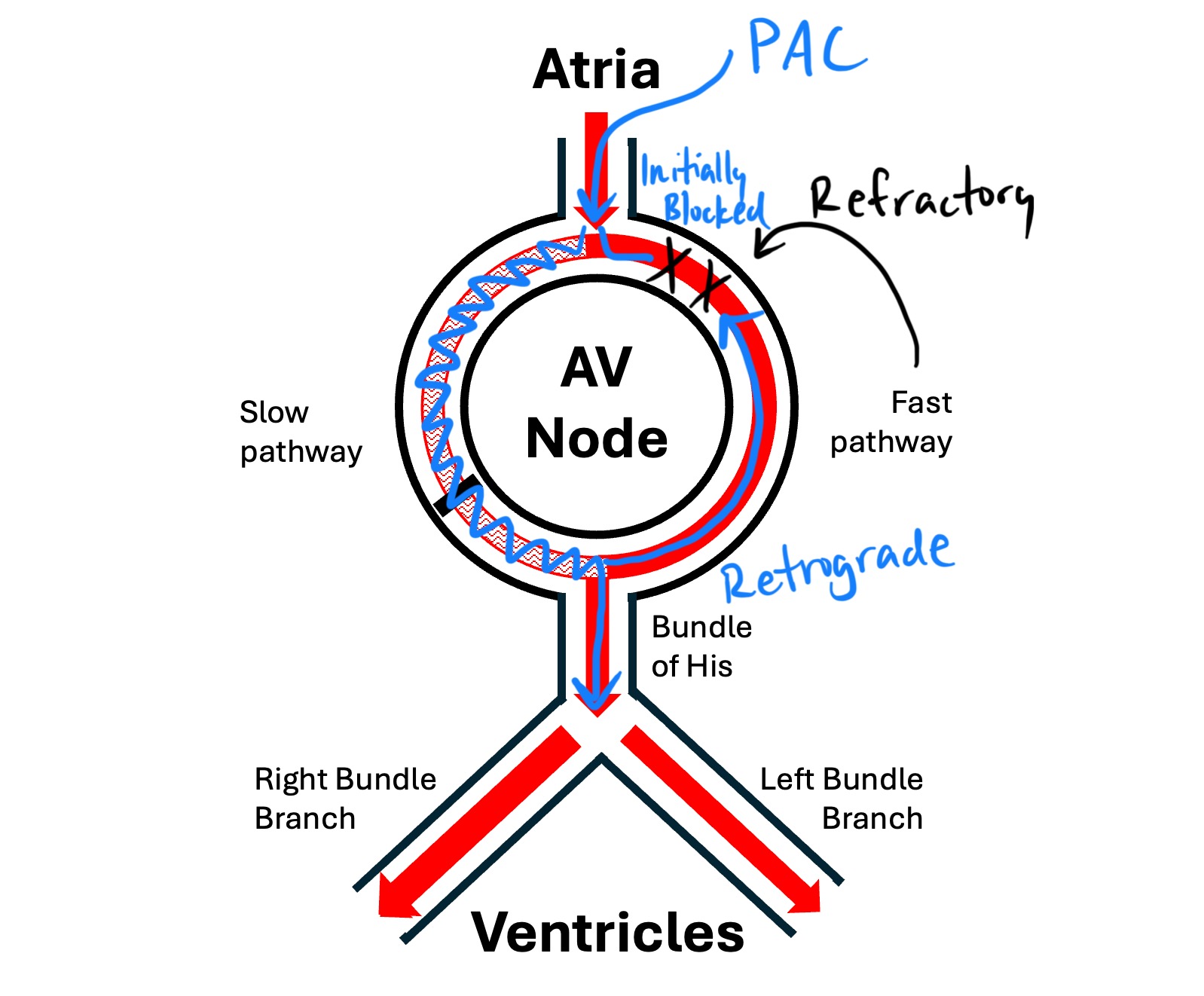
AVNRT requires a premature atrial beat (PAC) to initiate the reentrant circuit:
-
A PAC arrives early, when the fast pathway is still refractory from the preceding beat.
-
The impulse is blocked in the fast pathway and instead travels down the slow pathway, which has already recovered.
-
By the time the impulse reaches the base of the AV node via the slow pathway, the fast pathway has recovered, allowing retrograde conduction back up toward the atria.
-
This sets up a reentrant circuit:
-
Antegrade conduction down the slow pathway
-
Retrograde conduction up the fast pathway
-
This loop can sustain itself, firing the AV node repeatedly and sending each impulse down to the ventricles and back up to the atria—producing a regular narrow complex tachycardia.
Types of AVNRT
There are several recognized forms of AVNRT, but the two main ones are:
-
Typical AVNRT (slow-fast): Most common (90–95%). Slow antegrade, fast retrograde.
-
Atypical AVNRT (fast-slow or slow-slow): Less common. Often presents with different RP intervals and sometimes a less abrupt onset.
ECG Features of AVNRT
-
Regular narrow QRS complexes (unless there is aberrancy)
-
No visible P waves, or P waves buried in or just after the QRS (short RP interval)
-
Abrupt onset and termination
-
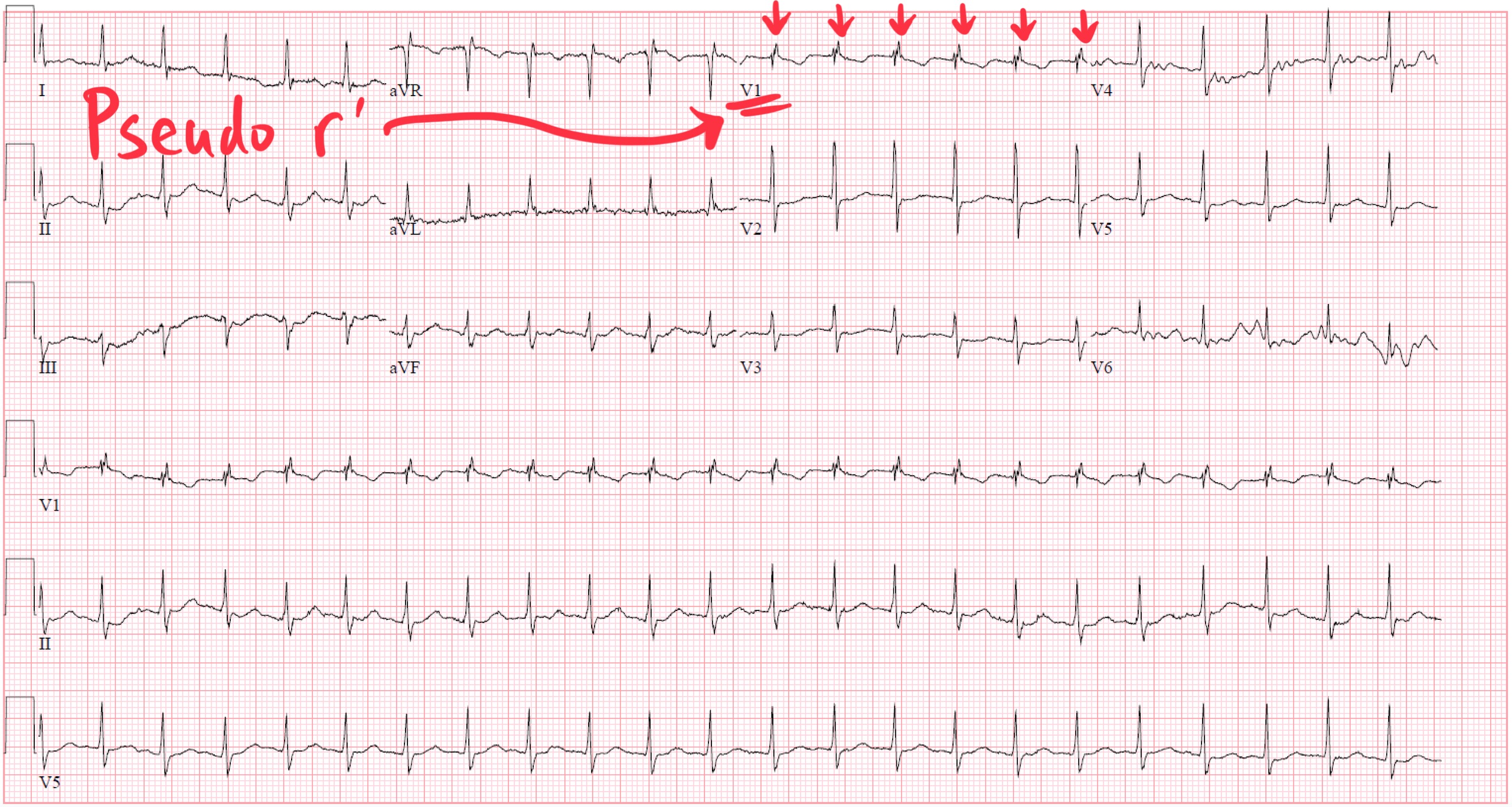
May see a pseudo R' in V1 or pseudo S wave in inferior leads (retrograde P wave)
Treatment Options and Their Mechanistic Basis
Understanding the reentrant circuit helps explain why certain treatments work (excluding cardioversion):
1. Vagal Maneuvers
-
Stimulate the parasympathetic nervous system
-
Slow AV nodal conduction and prolong AV nodal refractory periods
-
This interrupts the circuit, particularly blocking the slow pathway
2. Adenosine
-
A purine nucleoside that causes transient AV nodal block via A1 receptors
-
Temporarily halts conduction in both fast and slow pathways
-
Terminates AVNRT in most cases within seconds of administration
-
Useful diagnostically and therapeutically
3. Beta Blockers / Calcium Channel Blockers
-
Slow conduction through the AV node and prolong recovery
-
May terminate or prevent recurrence of AVNRT
-
Especially helpful in patients with frequent episodes but no structural heart disease
4. Catheter Ablation
-
Curative therapy
-
Most commonly targets the slow pathway, since ablating the fast pathway carries a higher risk of complete heart block
-
Success rates exceed 95% with low complication rates
Clinical Takeaway
AVNRT is a reentrant rhythm that exploits dual conduction pathways within the AV node. It initiates when conduction conditions—especially following a premature atrial beat—favor travel down the slow pathway and retrograde return through the fast pathway. Treatments work by either slowing conduction, increasing refractoriness, or interrupting the reentry circuit altogether. When these measures fail or episodes recur, ablation of the slow pathwayoffers a highly effective solution.
Enjoy this style of lecture and looking to learn more? Click below to learn more about how you can join my complete ECG course.
ECG With Reid Academy
Accredited by the AMA, AAPA, ANCC, ACPE & more.
