
Two Diagnoses, One Tracing: A Case Review
Dec 02, 2025
![]()
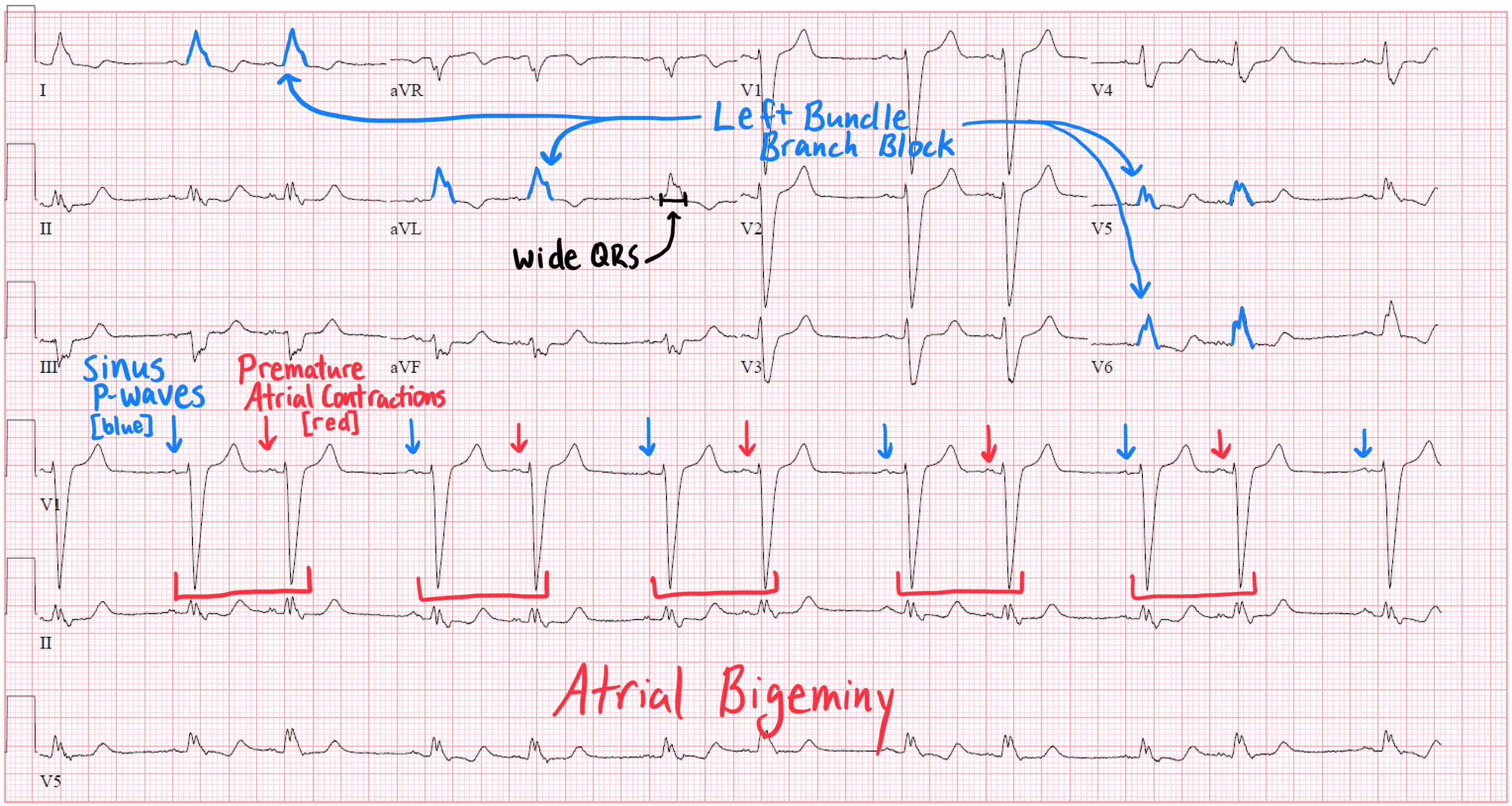
Interpreting ECGs in clinical practice is rarely about identifying a single abnormality. More often, the tracing is a layered story—atrial findings, ventricular conduction patterns, repolarization changes, and rate-dependent phenomena all stacked together. This week’s ECG is a perfect example: atrial bigeminy coexisting with left bundle branch block (LBBB).
At first glance, it’s easy for the premature atrial contractions to dominate your attention—or for the LBBB morphology to overshadow everything else. But recognizing both processes simultaneously is what elevates ECG interpretation from pattern recognition to clinical reasoning.
In the associated lecture, I walk through this ECG step-by-step, highlighting the anatomy behind each finding and showing how a structured approach prevents you from missing important pathology.
Atrial Bigeminy: The Atrial Layer of the Story
Atrial bigeminy is defined by a repeating pattern: every sinus beat is followed by a premature atrial contraction (PAC). The result is group beating, a hallmark appearance created by alternating normal and early atrial depolarizations.
Here’s what to look for:
-
A consistent coupling interval: The PAC occurs at roughly the same distance from the preceding sinus P wave.
-
Altered P-wave morphology: The ectopic atrial focus produces a P wave that is often subtly different from the sinus P—earlier, slightly different axis, or embedded in the preceding T wave.
-
Group beating: The rhythm has a “paired” cadence—normal beat + premature beat—repeating in a predictable cycle.
Atrial bigeminy isn’t just a rhythm curiosity; it matters clinically because:
-
It may reflect atrial irritability from ischemia, stretch, sympathetic tone, or metabolic disturbance.
-
It alters AV nodal conduction dynamics.
-
It creates sequences of alternating diastolic filling, which may have hemodynamic effects in certain patients.
If you stop your interpretation here, you’ve caught the atrial abnormality—but you’ve missed half the picture.
Left Bundle Branch Block: The Ventricular Layer of the Story
The same ECG may also show LBBB, and this isn’t incidental. LBBB dramatically changes ventricular activation:
-
Septal activation reverses, depolarizing right-to-left.
-
The left ventricle depolarizes late, generating the characteristic widened QRS.
-
Repolarization abnormalities follow predictable directions, making ST-T interpretation more nuanced.
Classic ECG findings of LBBB include:
-
QRS ≥ 120 ms
-
Broad, notched R waves in I, aVL, V5–V6
-
Deep, broad S waves in V1–V2
-
Secondary ST-T abnormalities (appropriate discordance)
In the context of atrial bigeminy, the LBBB morphology persists despite the premature atrial impulses, reinforcing that the conduction delay is fixed (not rate-related).
Again—recognizing LBBB alone is easy. Recognizing it on top of an atrial ectopic rhythm requires slowing down and thinking anatomically.
Enjoy this style of lecture and looking to learn more? Click below to learn more about how you can join my complete ECG course.
ECG With Reid Academy
Accredited by the AMA, AAPA, ANCC, ACPE & more.
