
Atrial Fibrillation with WPW Syndrome (Pre-excited AFib)
Jun 26, 2026Pre-excited atrial fibrillation is one of the few rhythm diagnoses in ECG interpretation where mechanism immediately informs risk. The arrhythmia itself is simply AF—but the presence of an accessory pathway radically changes how ventricular activation occurs and how dangerous the rhythm becomes. Understanding the electrophysiology explains every ECG feature you see.
The Core Problem: No AV Nodal Filter
In typical AF, the AV node acts as a physiologic choke point, limiting ventricular response despite chaotic atrial activity.
In pre-excited AF, the accessory pathway (AP) bypasses the AV node entirely. Because the AP conducts rapidly and without decrement, a significant portion of atrial impulses reach the ventricles at high rates.
The result: ventricular rates that can exceed 250–300 bpm, distributed in a completely irregular pattern.
Mechanism of Ventricular Activation: Competing Wavefronts
Each atrial impulse can conduct down:
-
The accessory pathway, producing early, slow, slurred ventricular activation through myocardium
-
The AV node–His–Purkinje system, producing later, rapid ventricular activation
These competing depolarization fronts create beat-to-beat fusion, but unlike classic WPW sinus rhythm, the timing varies with every atrial cycle length. That variability is what generates the hallmark ECG appearance.
ECG Findings to Recognize
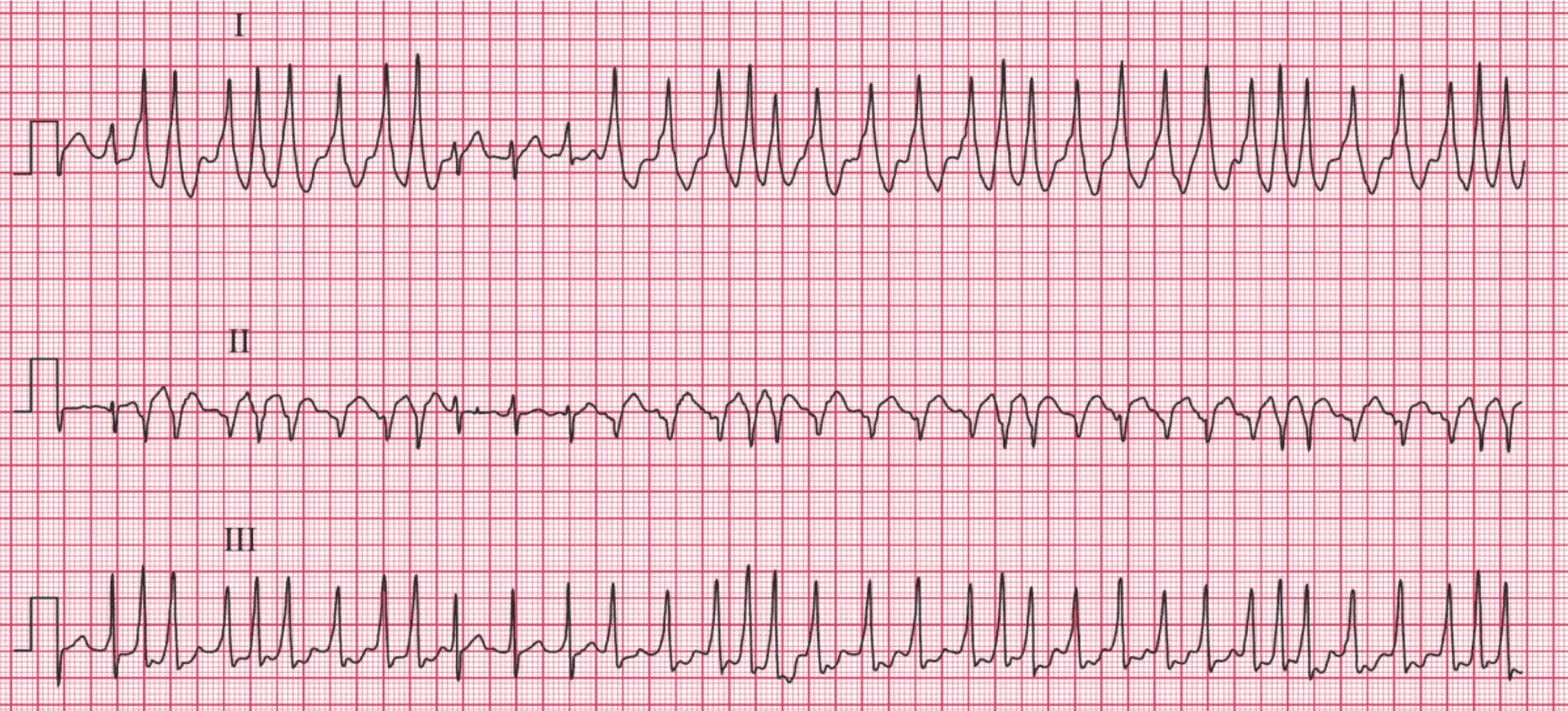
1. Irregularly Irregular, but Extremely Fast
Rates typically exceed 180 bpm and often approach 250–300 bpm. Unlike AVN-filtered AF, there are no long pauses and the R-R variability is chaotic rather than clustered.
2. Wide QRS Complexes with Variable Morphology
Because each ventricular activation is a fusion beat between AP conduction and AV nodal conduction, the QRS width and shape fluctuate beat-to-beat.
Key point: This variability differentiates it from monomorphic VT.
More pre-excited beats → broader, more bizarre morphologies
More His–Purkinje competition → narrower beats
The spectrum often ranges from:
-
fully pre-excited, very wide complexes
-
to partially fused complexes
-
to nearly normal-appearing QRS complexes
3. Absence of Organized P Waves
Consistent with AF, atrial activity is chaotic, but because conduction is partially or entirely bypassing the AV node, you may see rapid fibrillatory waves best in V1.
https://manualofmedicine.com/ecgs/ecg-case-80-atrial-fibrillation-and-wpw-syndrome/
Why It’s Dangerous
If the pathway can conduct impulses at extremely short intervals, the ventricular response can accelerate to rates capable of degenerating into ventricular fibrillation. Pathways with antegrade refractory periods < 250 ms are particularly concerning.
This mechanism also explains why:
-
AV nodal blockers (beta blockers, diltiazem, verapamil, adenosine) are contraindicated.
They eliminate the AV nodal “competition,” allowing more impulses to traverse the AP → further pre-excitation → faster ventricles → greater VF risk. -
Procainamide or ibutilide are preferred, as they prolong AP refractory period and slow conduction through the pathway.
Enjoy this style of lecture and looking to learn more? Click below to learn more about how you can join my complete ECG course.
ECG With Reid Academy
Accredited by the AMA, AAPA, ANCC, ACPE & more.
