
Why T Waves Peak in Hyperkalemia: Cellular Mechanisms and ECG Correlates
May 23, 2025One of the earliest and most recognized ECG manifestations of hyperkalemia is the peaked T wave—a tall, narrow, and symmetric repolarization wave that often raises clinical alarm. But why does excess extracellular potassium cause this specific change?
To truly understand the peaked T wave, we must zoom in to the cellular level, examining how elevated serum potassium (K⁺) influences the cardiac action potential, particularly during repolarization, and how this altered electrophysiology projects onto the surface ECG.
Related topics:
Resting Membrane Potential and Extracellular Potassium
Cardiac myocytes maintain a resting membrane potential (RMP) primarily via the K⁺ gradient between the intracellular (~150 mEq/L) and extracellular (~3.5–5.0 mEq/L) spaces.
-
RMP ≈ –90 mV, established by outward K⁺ leak currents through inward rectifier K⁺ channels (IK1).
-
When extracellular K⁺ increases, the gradient narrows, making the RMP less negative (i.e., partially depolarized).
This shift has profound effects on the excitability and repolarization behavior of the cell.
The Action Potential in Hyperkalemia
Phase 0: Slowed Depolarization
-
Mild-to-moderate hyperkalemia inactivates fast Na⁺ channels due to a less negative RMP.
-
This slows phase 0 depolarization, leading to widened QRS complexes in more advanced stages.
Phase 3: Accelerated Repolarization
-
Elevated extracellular K⁺ increases K⁺ conductance, particularly through delayed rectifier K⁺ channels (IKr, IKs). Its allosteric effects actually improve IK efflux conduction velocities, speeding up repolarization as K exits the cell.
-
This leads to a steeper and faster phase 3 repolarization slope.
⚡ Faster repolarization = taller and narrower T waves
These changes occur before QRS widening, making peaked T waves the earliest ECG clue in hyperkalemia.
ECG Correlation: The Peaked T Wave
The T wave on ECG represents ventricular repolarization. Under normal conditions:
-
Repolarization is a relatively slow, dispersed process.
-
The T wave is broad and asymmetrical.
In hyperkalemia:
-
Enhanced K⁺ efflux causes a rapid, synchronous repolarization.
-
The T wave becomes tall, narrow, and symmetric.
This "peaking" is especially prominent in the precordial leads (V2–V4), where myocardial voltage vectors are most visible.

Clinical Progression on ECG
Hyperkalemia progresses in a predictable electrophysiologic sequence, typically:
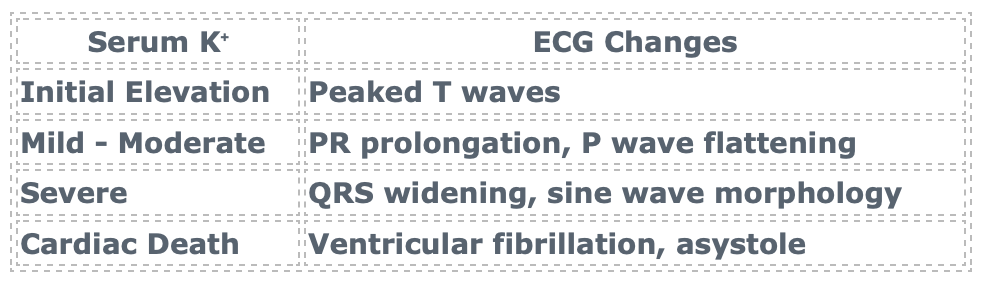
The peaked T wave is the earliest and most reversible sign, making its recognition critical in clinical practice.
Summary: Mechanism of Peaked T Waves
-
Hyperkalemia reduces the RMP, impairing Na⁺ channel availability and excitability.
-
Increased extracellular K⁺ enhances K⁺ conductance, especially during repolarization.
-
This leads to faster phase 3 repolarization, generating tall, narrow, symmetric T waves.
-
These ECG changes correlate precisely with altered action potential kinetics at the cellular level.
Enjoy this style of lecture and looking to learn more? Click below to learn more about how you can join my complete ECG course.
ECG With Reid Academy
Accredited by the AMA, AAPA, ANCC, ACPE & more.
