
Junctional Escape Beats: Evaluating the Underlying Problem
Dec 10, 2025A junctional escape beat is not a dysrhythmia—it is the myocardium rescuing the ventricles when the normal hierarchy fails. Whenever you see a junctional escape, your diagnostic focus should immediately shift to why the junction had to fire.
Every junctional escape originates from one of three mechanisms:
-
Sinus node failure (impulse not generated or not exiting the SA node)
-
AV conduction failure (impulse generated but blocked before His–Purkinje)
-
A compensatory pause following a premature beat (PAC/PVC creating a long-enough interval for the junction to “escape”)
Understanding which mechanism is present is the key to interpreting the rhythm and identifying pathology.
The Physiology: The Junction Fills a Timing Void
The AV junction (typically the AV node/His region) has an intrinsic firing rate around 40–60 bpm. As long as the sinus node sends impulses on time, the junction remains suppressed.
But if the junction waits longer than its intrinsic escape interval (~1.0–1.5 seconds) and receives no incoming depolarization, it takes over.
That “long pause” is your diagnostic goldmine.
Step 1: Examine the Pause Before the Escape Beat
A. Sinus Node Failure (Sinus Arrest or SA Exit Block)
Here the problem is with impulse formation or impulse exit at the SA node.
-
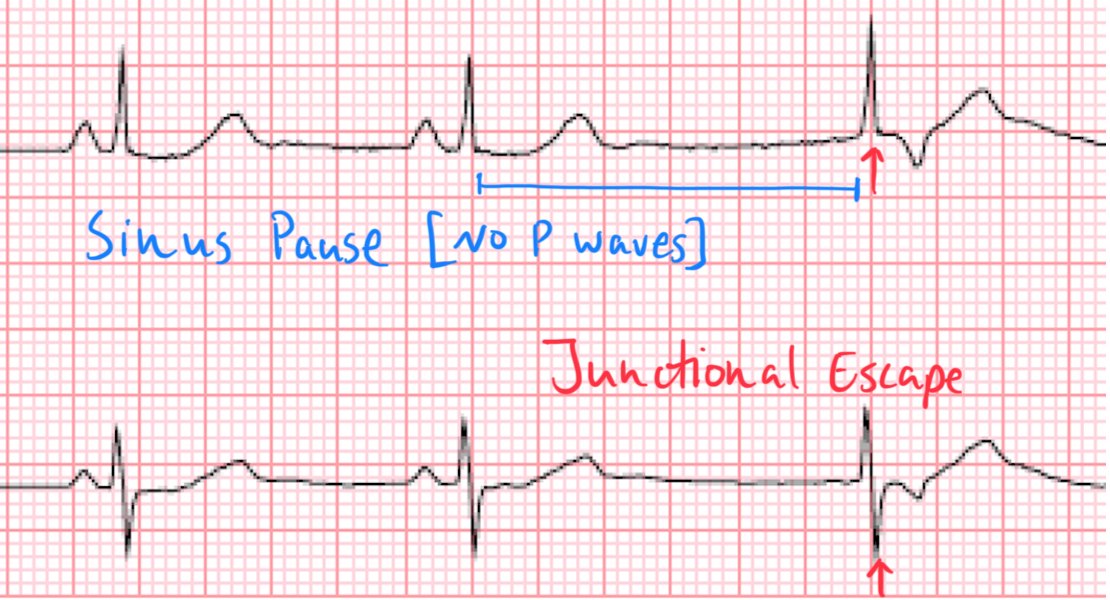
Sinus Pause or Arrest:
The sinus node simply fails to fire.-
No P wave where one should be
-
Pause is not a multiple of the baseline P–P interval
-
Junctional escape follows the prolonged gap
-
-
SA Exit Block:
The sinus node fires normally, but impulses fail to leave the node.-
P–P intervals occur in exact multiples of the intrinsic sinus cycle length
-
The pause is “too perfect” to be random
-
Escape beat appears after the blocked cycle
-
These are disorders of impulse formation or exit.
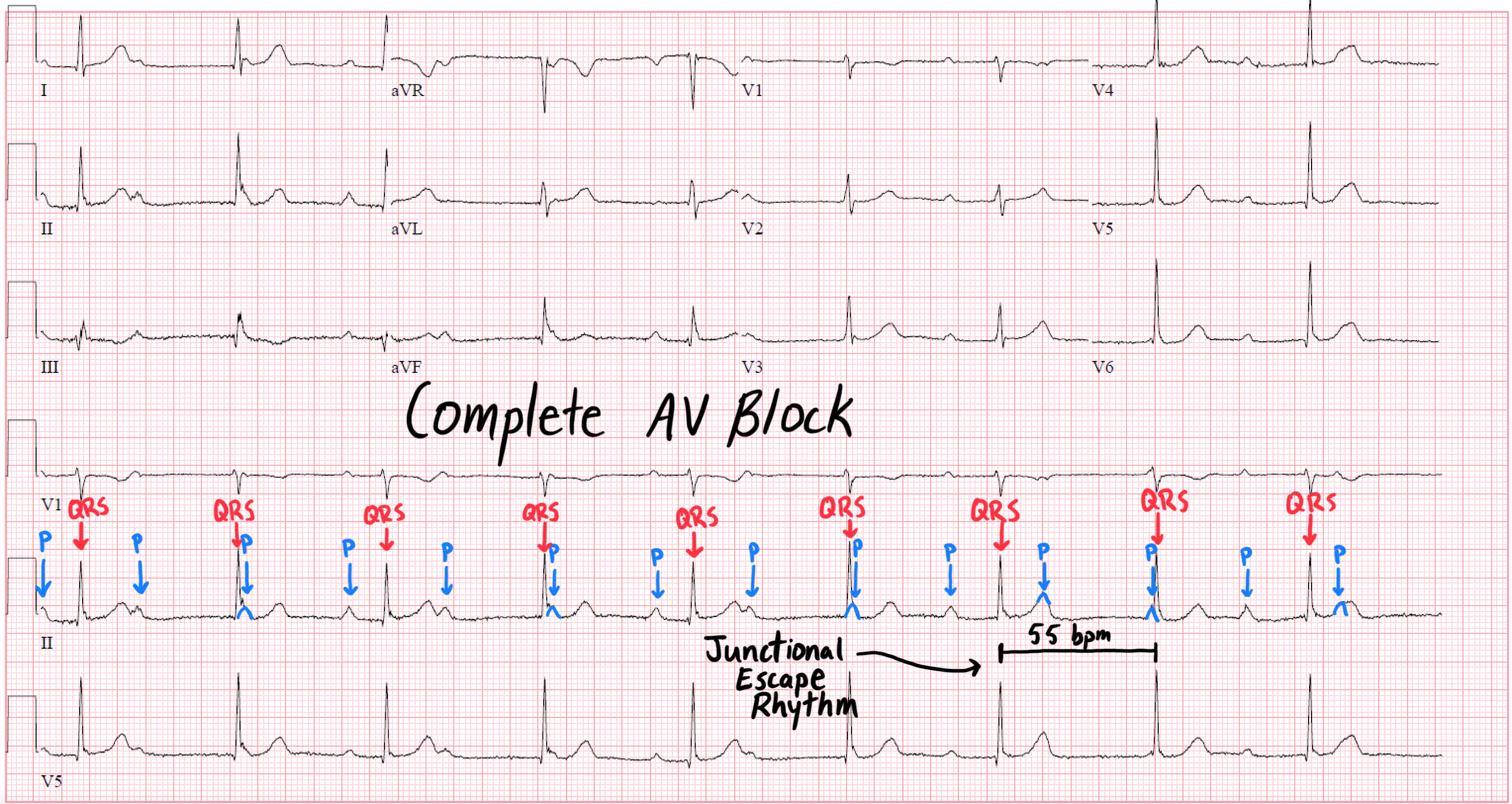
B. AV Conduction Failure (AV Block)
Here the sinus node fires appropriately, but impulses never reach the ventricles.
-
A P wave is present but not followed by a QRS.
-
The junctional escape beat follows because the atrial signal never reached the His bundle.
Key distinctions:
-
Persistent atrial activity = this is not an SA node problem
-
PR intervals before the block and QRS width help localize AV nodal vs infranodal disease vs complete heart block
This is a disorder of impulse conduction.
C. Compensatory Pause After a Premature Beat (PAC or PVC)
This third mechanism is often overlooked.
A premature atrial or ventricular contraction can trigger a pause long enough for the junction to escape:
-
PAC with a post–extrasystolic pause:
The premature P arrives early, resets the sinus node, and the next normal sinus beat is delayed.
If the delay exceeds the junctional escape interval → escape beat occurs.
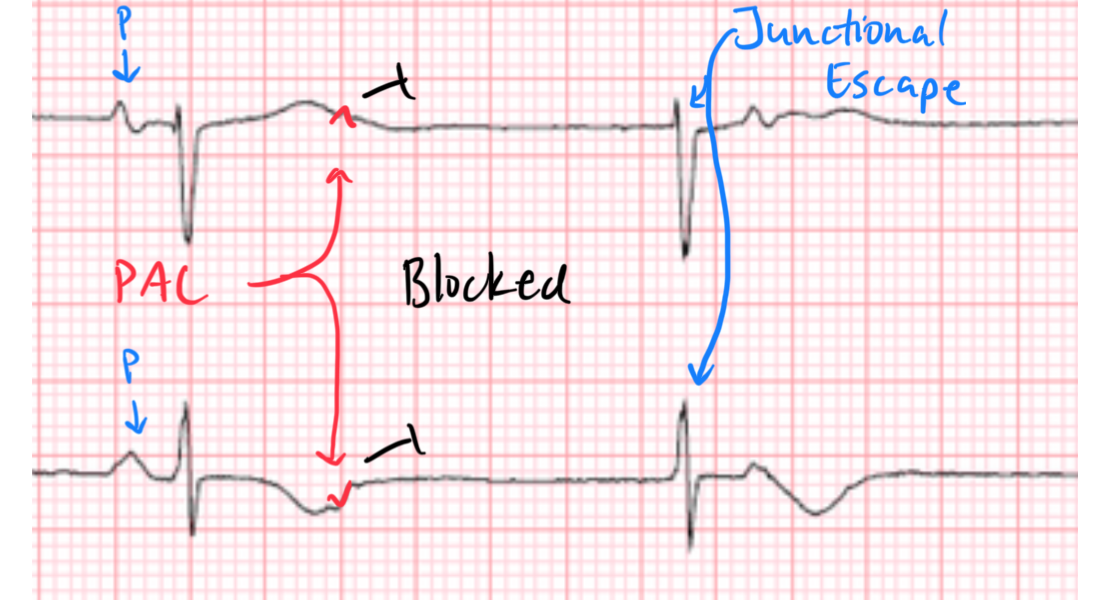
Here we have an example of a non-conducted (blocked) PAC that resets the SA node, leading to a Junctional Escape beat.
-
PVC with a full compensatory pause:
The sinus node continues on time, but the ventricles are refractory and don’t respond.
After a long post-PVC pause, the junction fires because its intrinsic timer expires.
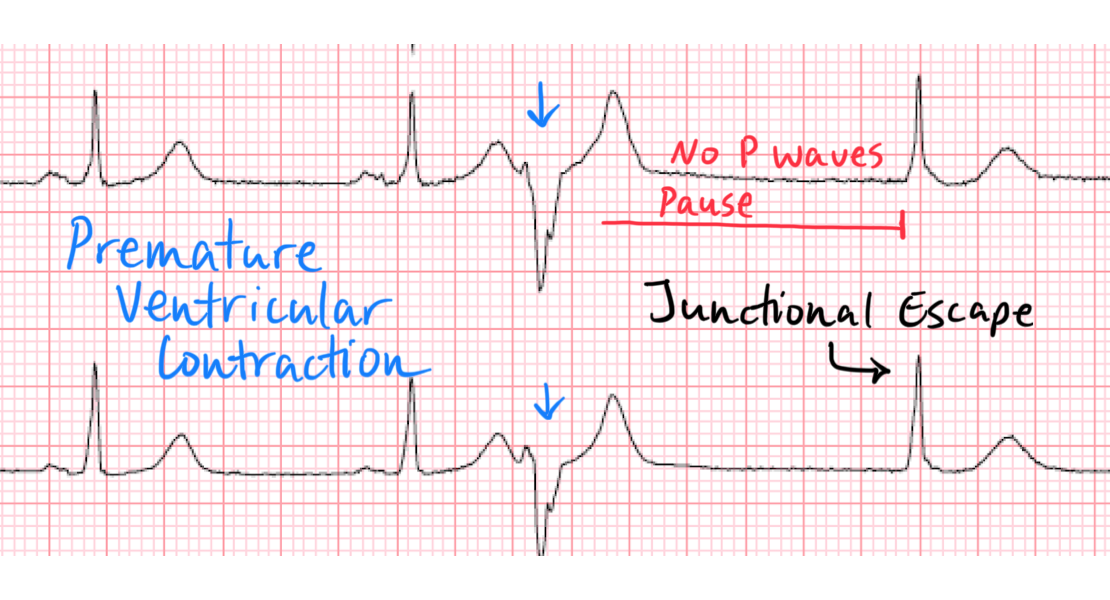
Clues this is the mechanism:
-
A premature beat is clearly seen before the escape
-
The pause length matches a post-extrasystolic interval rather than sinus node dropout
-
After the junctional escape, the sinus rhythm typically resumes normally
This is a timing-reset phenomenon, not a conduction disease.
Step 2: Inspect Atrial Activity Carefully
This is the most discriminating step.
Ask:
-
Is atrial activity absent before the escape? → Sinus arrest or SA exit block
-
Is atrial activity present but non-conducted? → AV block
-
Is atrial activity present but interrupted by a PAC? → PAC with compensatory pause
-
Is the pause preceded by a PVC? → post-PVC pause causing escape
Pay special attention to lead II and V1 for small or hidden P waves.
Step 3: Evaluate Baseline Sinus Function
Even outside the pause:
-
Is the sinus rate too slow for the clinical situation?
-
Is there sinus arrhythmia or chronotropic incompetence?
-
Is there long-standing bradycardia?
These findings point toward underlying sinus node disease.
Step 4: Identify Reversible Contributors
Many junctional escapes occur because of transient suppression of the sinus node or AV node.
Look for:
-
Medications: beta blockers, CCBs, digoxin, amiodarone
-
Vagal surges (pain, nausea, sleep, carotid sinus stimulation)
-
Ischemia, especially RCA/SAN artery ischemia
-
Metabolic causes: hyperkalemia, hypoxia, acidemia
-
Post-tachycardia conversion pauses
-
Congenital or age-related fibrosis of conduction tissue
If the escape beat is new, presume a reversible cause until proven otherwise.
Enjoy this style of lecture and looking to learn more? Click below to learn more about how you can join my complete ECG course.
ECG With Reid Academy
Accredited by the AMA, AAPA, ANCC, ACPE & more.
