
Isorhythmic AV Dissociation from Sinus Arrhythmia
Dec 06, 2025Isorhythmic AV dissociation is one of those ECG findings that looks more arcane than it actually is. At first glance, it can mimic AV block, retrograde atrial activation, or even a wandering pacemaker. But when you approach it through physiology—specifically, the competing intrinsic rates of the SA node and AV junction—the tracing becomes remarkably intuitive.
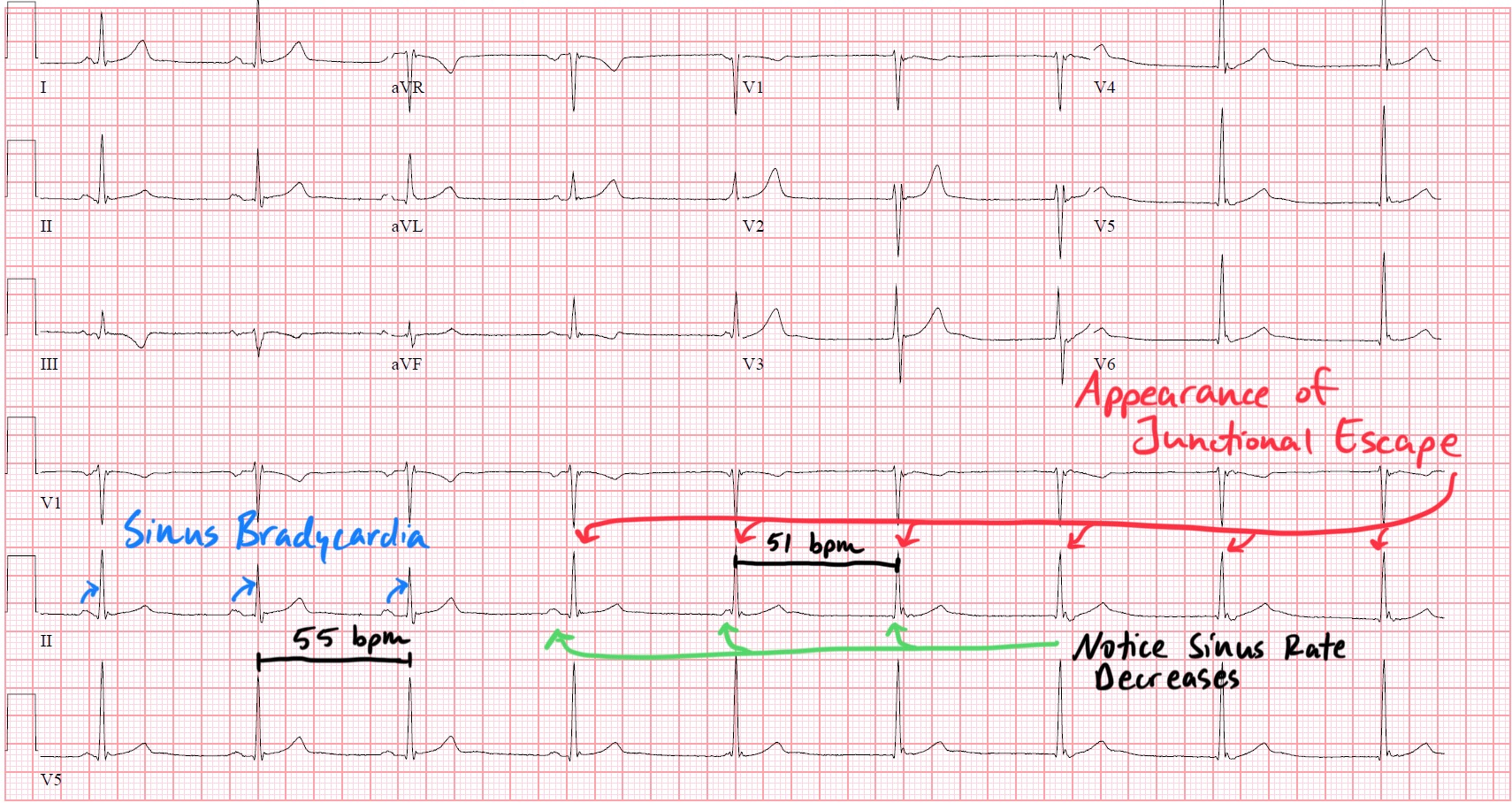
The most common clinical setting is sinus arrhythmia with vagally mediated SA node slowing. During normal respiration or heightened vagal tone, the SA node’s firing interval can lengthen just enough that it briefly relinquishes its leadership role. When that pause reaches the intrinsic escape interval of the AV junction, a junctional escape rhythmemerges—not because conduction is impaired, but because the timing simply favors the subsidiary pacemaker.
This creates the hallmark pattern:
two pacemakers firing at nearly identical rates, neither truly overriding the other.
The result is dissociation without dominance: P waves wander across the QRS complexes, sometimes preceding them, sometimes falling inside them, and sometimes appearing just after. The atria and ventricles are not blocked from each other—they are merely out of sync by coincidence of rate.
The ECG reveals the physiology cleanly if you know where to look:
-
PP intervals demonstrate respiratory variation, confirming the sinus node is slowing and accelerating in a predictable pattern.
-
QRS complexes remain narrow, signaling that ventricular activation is originating from a stable junctional focus rather than from aberrancy.
-
The P–QRS relationship shifts beat to beat, reflecting two clocks with nearly identical but not identical rates.
-
Depending on the patient’s conduction system, you may see fusion of atrial and ventricular timing, or periods when sinus impulses momentarily capture the ventricles again.
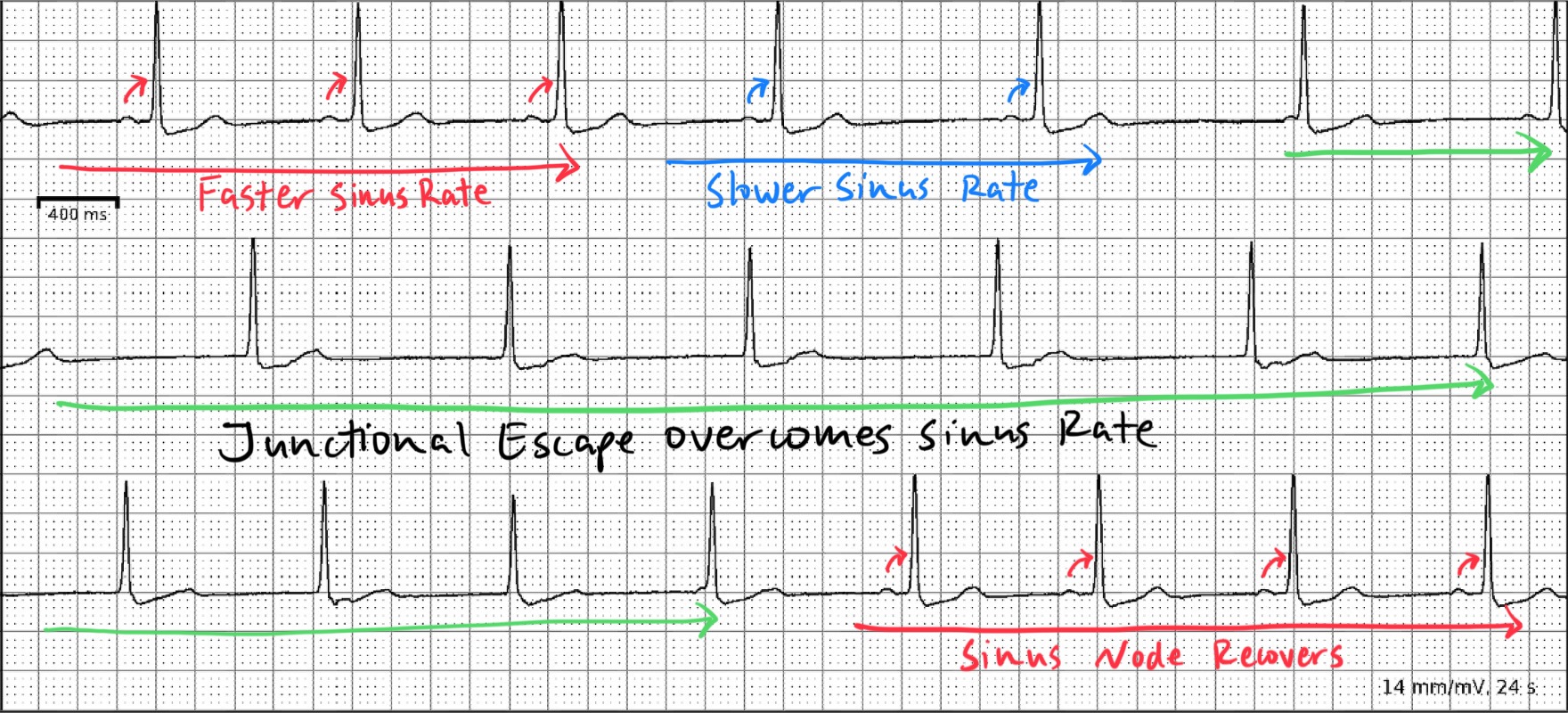
The critical distinction—especially for physicians confronted with bradycardia—is that this is not an AV block. Conduction is intact; the physiology is rate competition. The SA node is simply firing too slowly for brief intervals, allowing the junction to express itself until sinus rate rises again and reclaims control.
Clinically, recognizing this protects patients from unnecessary pacemaker implantation and helps you correctly attribute bradycardic episodes to vagal tone, medication effects, or normal physiologic variability rather than conduction system disease.
Enjoy this style of lecture and looking to learn more? Click below to learn more about how you can join my complete ECG course.
ECG With Reid Academy
Accredited by the AMA, AAPA, ANCC, ACPE & more.
