
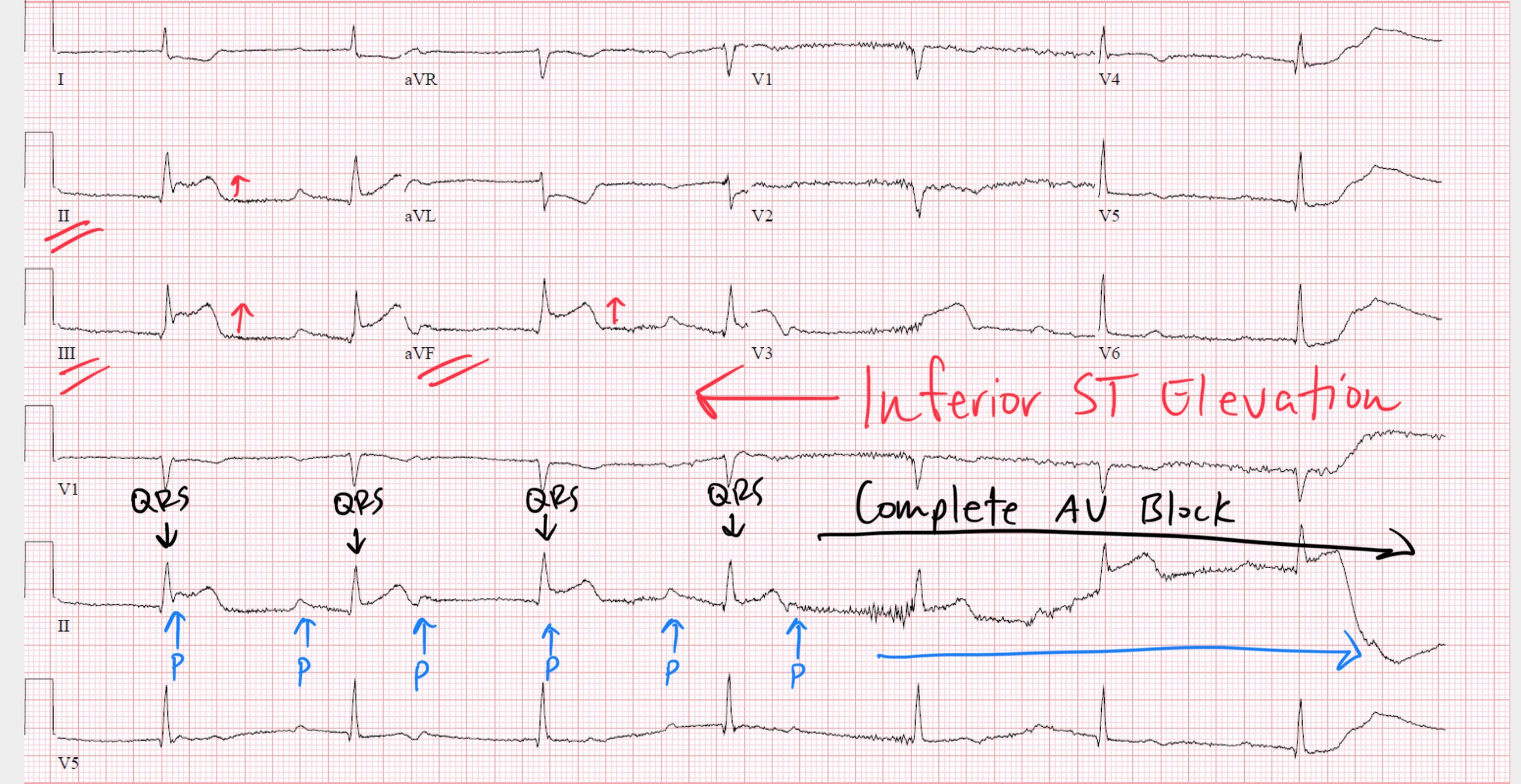
Inferoposterior STEMIs and Complete Heart Block: A Look at AV Node Anatomy and RCA Supply
Jun 04, 2025Complete heart block—or third-degree AV block—is a feared complication of ST segment elevation myocardial infarction (STEMI), particularly when the infarct involves the inferior or posterior walls of the heart. This pattern is not random. It’s grounded in the anatomical relationship between the right coronary artery (RCA) and the atrioventricular (AV) node.
In this article, we explore why inferior and posterior STEMIs are disproportionately associated with AV conduction disturbances, with a focus on vascular anatomy, nodal blood supply, and the electrophysiological consequences of ischemia.
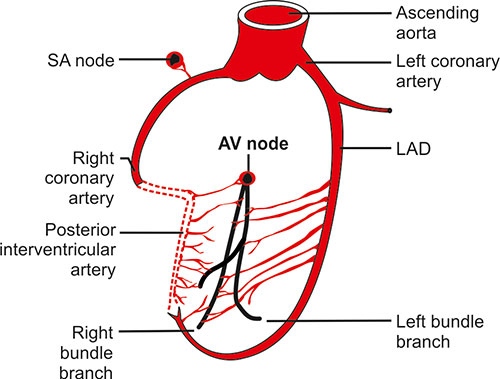
The AV Node: Central to Conduction
The atrioventricular node is a critical conduction structure that:
-
Delays conduction from atria to ventricles, allowing for appropriate ventricular filling
-
Filters out excessively rapid atrial impulses (such as during atrial fibrillation)
-
Serves as the only normal electrical bridge between the atria and ventricles
Its function depends on consistent perfusion, primarily from the AV nodal artery—a small but vital vessel that supplies this compact, high-stakes region of conduction tissue.
RCA and AV Node: A Close Vascular Relationship
In approximately 85–90% of individuals, the right coronary artery gives rise to the AV nodal artery, often at the level of the crux of the heart—where the atrial and ventricular septa meet near the coronary sinus.
As a result:
-
Inferior STEMIs, which typically result from proximal or mid-RCA occlusion, often involve the AV nodal artery.
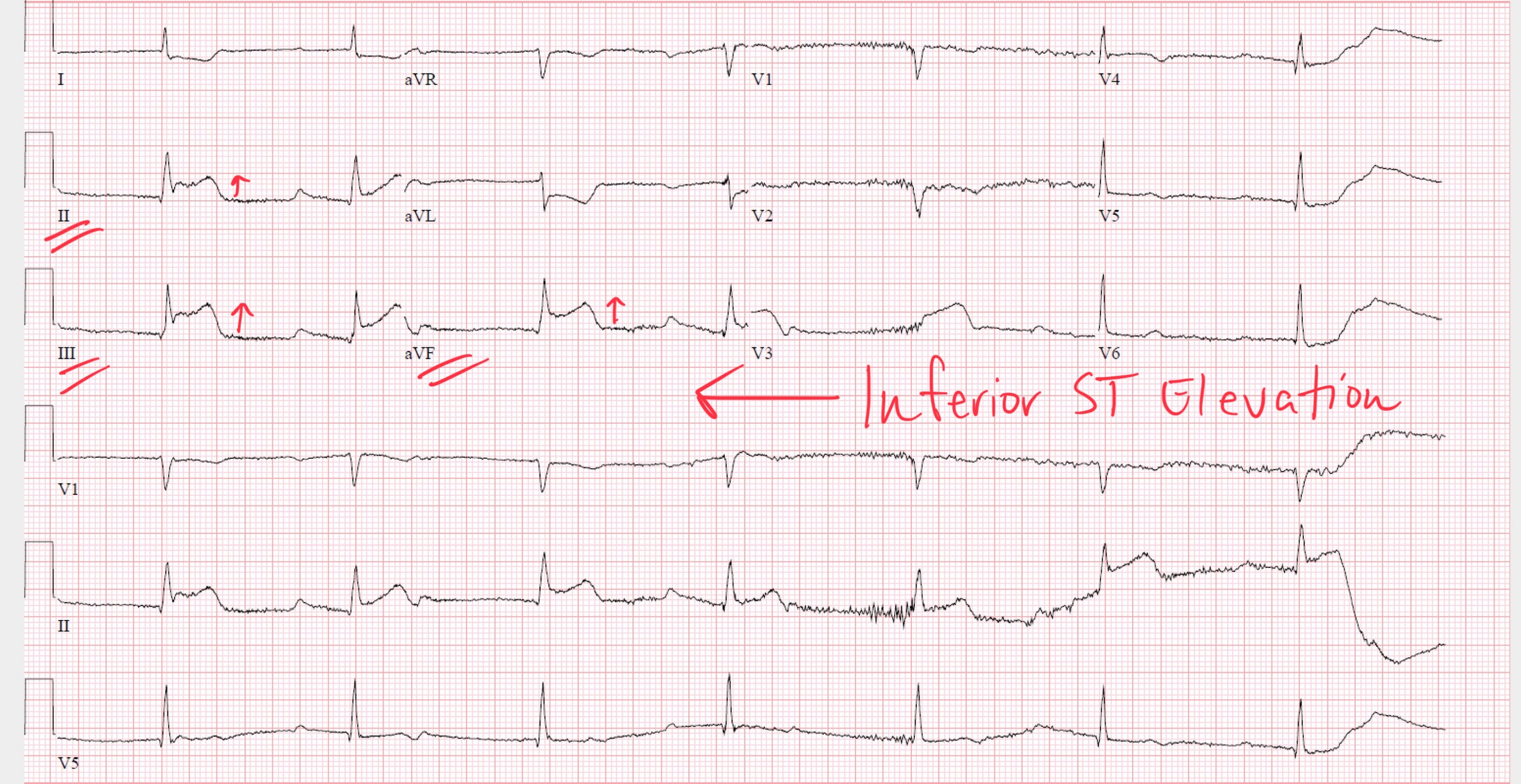
-
Posterior wall involvement—commonly an extension of an inferior infarct—can further compromise perfusion to conduction structures situated along the posterior septum and crux.
Thus, RCA occlusion doesn’t just injure the inferior wall of the left ventricle, but also directly endangers the AV node.
Electrophysiological Consequences of AV Node Ischemia
Ischemia of the AV node results in:
-
Slowed conduction velocity
-
Prolongation of PR interval (first-degree AV block)
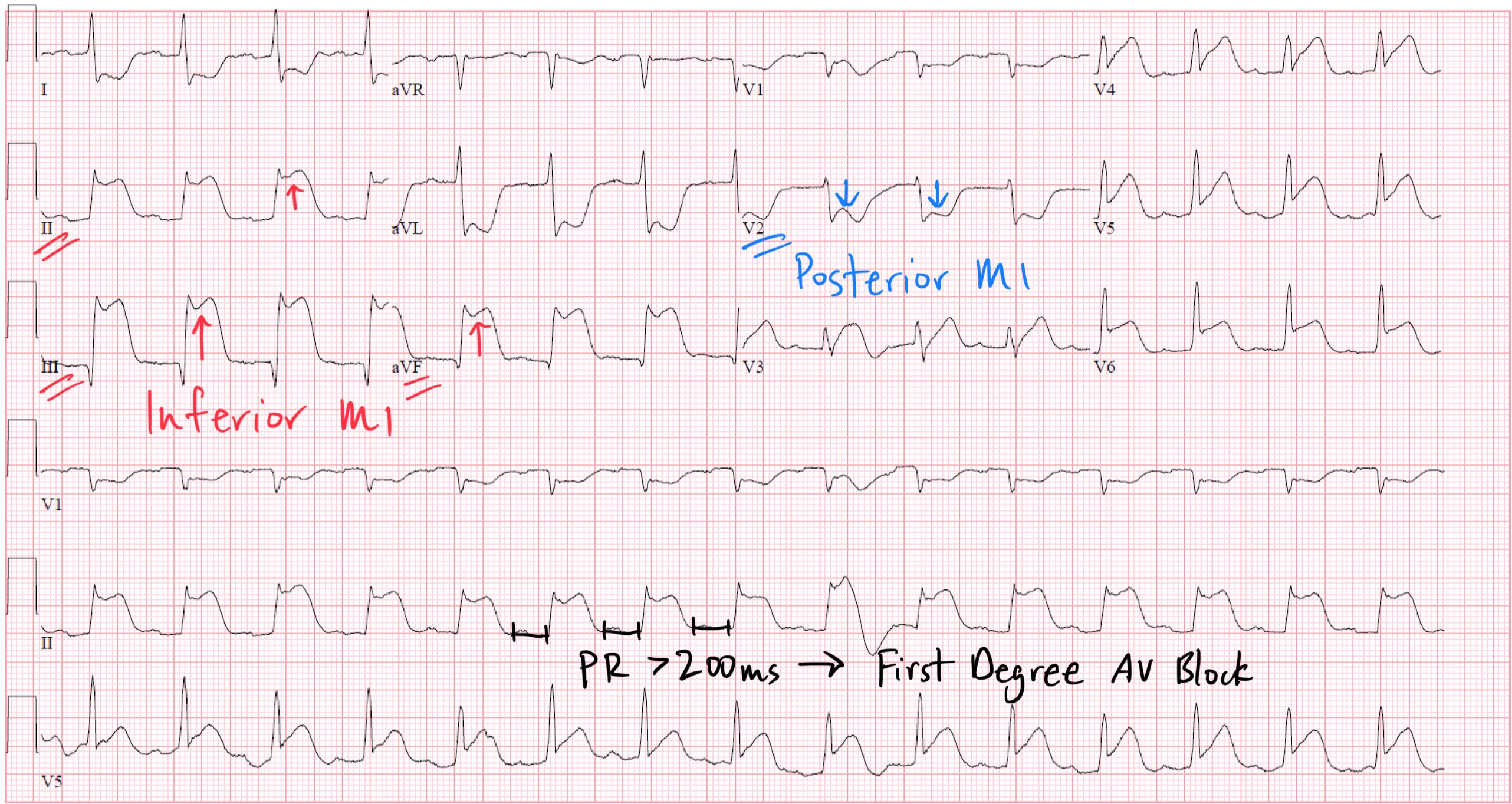
-
Intermittent failure of conduction (second-degree AV block, particularly Mobitz type I)
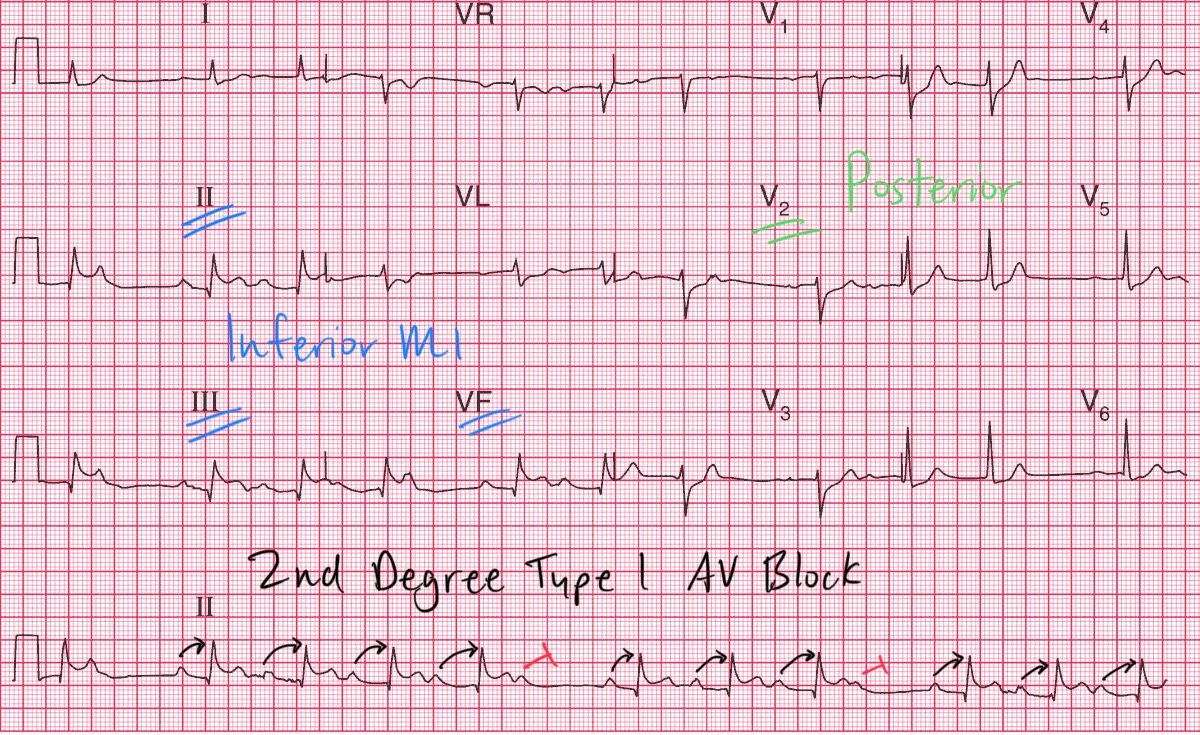
https://manualofmedicine.com/ecgs/ecg-interpretations/inferior-posterior-stemi-second-degree-type-i-av-block-wenckebach/
-
Complete conduction block (third-degree AV block)
This progression is especially common in inferior infarctions due to the relatively high ischemic vulnerability of the AV node when its blood supply is interrupted.
Contrast with Anterior STEMIs
While anterior STEMIs (typically due to left anterior descending artery occlusion) can cause bundle branch blocks or fascicular blocks, they are less likely to cause AV nodal block unless:
-
The infarction is massive and involves the basal septum
-
There is extensive damage to the His-Purkinje system, beyond the AV node
This is because the AV node is not typically supplied by the LAD in most individuals.
Clinical Implications of AV Block in Inferior MI
-
AV block in inferior MI is often transient and nodal in origin.
-
Vagal tone and ischemia are reversible contributors.
-
These blocks often resolve with reperfusion, and pacemaker support is usually temporary.
In contrast, AV block in anterior MI—when it does occur—is usually due to extensive infarction of the conduction system below the AV node and has a poorer prognosis, often requiring permanent pacing.
Clinical Takeaway
The reason complete heart block occurs more frequently in inferior and posterior STEMIs is anatomical: the AV node receives its primary blood supply from the right coronary artery, which is commonly the culprit vessel in these infarctions. When the RCA is occluded, both myocardial tissue and the conduction system become ischemic, and the delicate AV node may cease to function properly—leading to high-grade AV block.
Understanding this relationship is essential for anticipating conduction disturbances in patients with inferior STEMI, interpreting AV block patterns, and making informed decisions about temporary pacing and reperfusion strategy.
Enjoy this style of lecture and looking to learn more? Click below to learn more about how you can join my complete ECG course.
ECG With Reid Academy
Accredited by the AMA, AAPA, ANCC, ACPE & more.
