
Group Beating on ECG: Differentiating the Mechanisms
Dec 08, 2025One of the most deceptively simple patterns in ECG interpretation is group beating—clusters of two or more beats separated by a pause, repeating in a predictable cadence. It’s a pattern that instantly catches the eye, yet the underlying physiology can be dramatically different depending on where the problem originates.
Two of the most common causes of group beating are:
-
Atrial bigeminy
-
Second-degree AV block (especially Mobitz I)
On paper, they can look eerily similar. But clinically, they couldn’t be more different. One arises from premature atrial activity, the other from impaired AV nodal conduction. This is where an anatomical approach becomes essential: follow the atria → AV node → His-Purkinje → ventricles sequence, and the diagnosis often becomes obvious.
This week’s post takes a deeper look at group beating—what it is, why it happens, and how to reliably separate atrial bigeminy from second-degree AV block when they produce nearly identical surface patterns.
What Exactly Is Group Beating?
Group beating refers to the ECG appearance where beats are “clustered”:
-
A sequence of two or more consecutive conducted beats
-
Followed by a pause
-
With the cycle then repeating
-
Creating the visual impression of groups of beats marching across the ECG
Group beating is not a diagnosis—it’s a pattern, one that can be generated by abnormalities in atrial firing, AV nodal conduction, or even concealed conduction.
To understand it, we must ask the anatomical questions:
-
What are the atria doing?
-
What is the AV node doing?
-
What are the ventricles doing?
When you anchor yourself in the conduction system’s structure, the pattern becomes easy to decode.
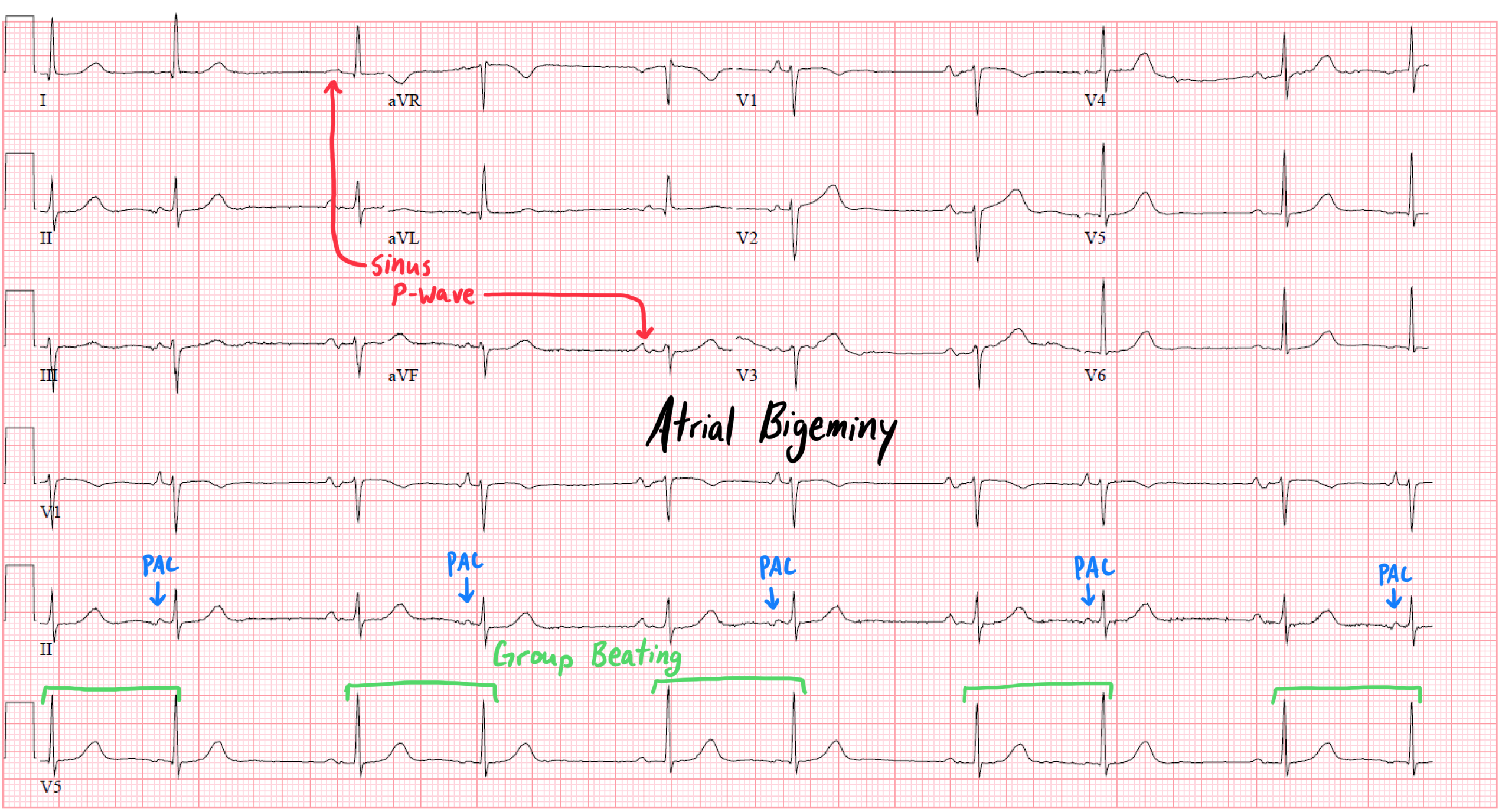
Atrial Bigeminy: Group Beating from the Atria
In atrial bigeminy, the atria fire prematurely every other beat. The pattern is:
Sinus beat → premature atrial contraction (PAC) → pause → repeat
Why does this create group beating?
-
The PAC arrives early, often with an altered P-wave morphology.
-
After the PAC, there is typically a compensatory pause, resetting the sinus node’s rhythm.
-
This normal–early–pause sequence repeats, producing the grouped pairs.
Key features of atrial bigeminy:
-
P-wave morphology varies: the PAC’s P wave is different from the sinus P.
-
The coupling interval is fixed: the PAC occurs at the same time after each sinus beat.
-
The pause is due to resetting of sinus node timing, not AV nodal disease.
-
QRS complexes are usually narrow—unless an aberrancy (e.g., Ashman phenomenon) or bundle branch block coexists.
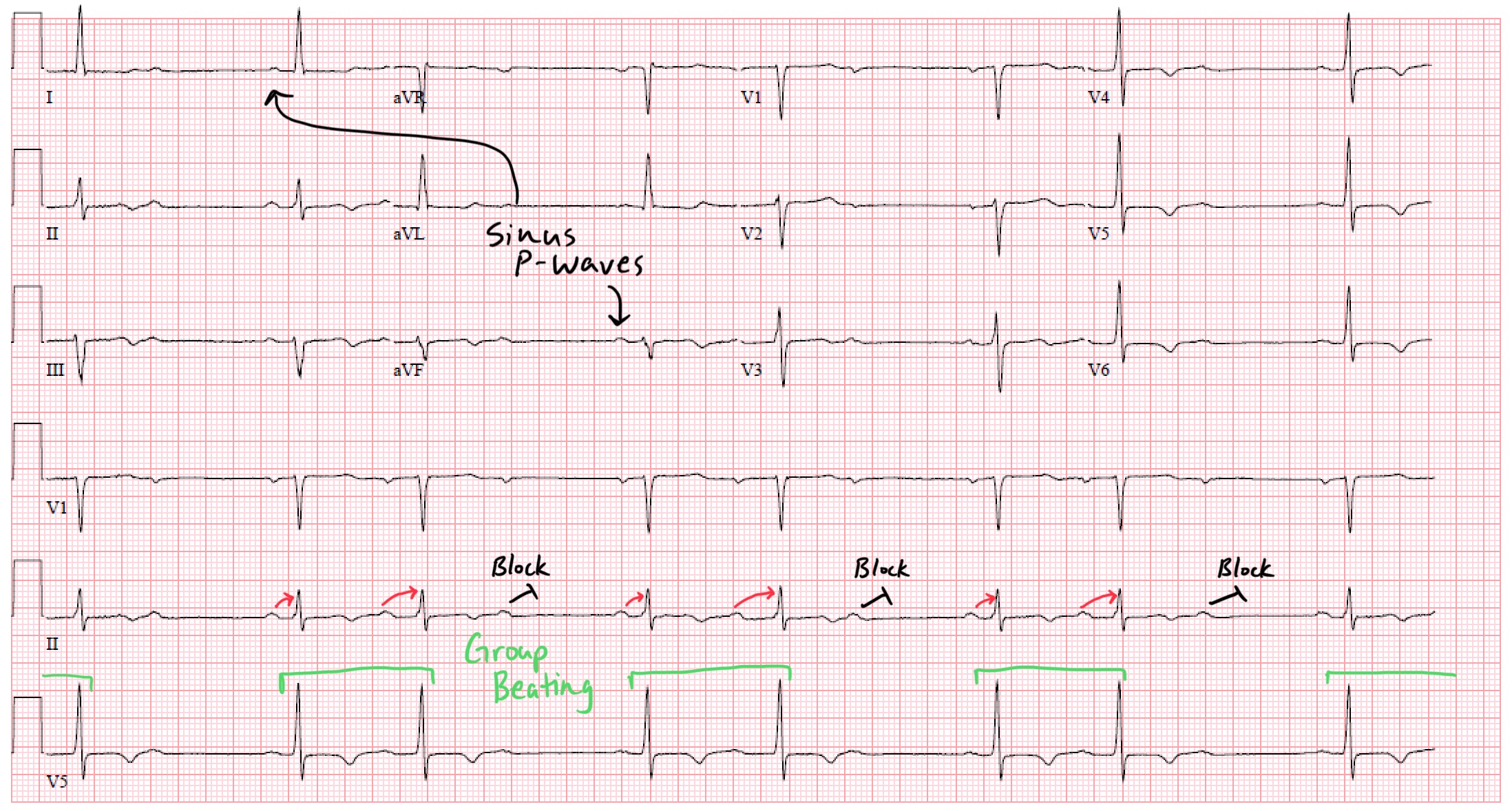
Second-Degree AV Block: Group Beating from the AV Node
Second-degree AV block—especially Mobitz I—can create nearly identical clusters of beats:
Conducted beat → conducted beat → dropped beat → pause → repeat
The pause creates the grouped appearance, but the mechanism is completely different.
Mobitz I (Wenckebach) pattern:
-
PR interval lengthens progressively
-
Eventually one P wave is blocked
-
After the dropped beat, the cycle resets
This creates a “group” of conducted beats followed by a dropped one.
Mobitz II:
These can also produce group beating, though the PR behavior differs.
Key features of second-degree AV block:
-
Every P wave is sinus in origin—no PACs.
-
The number of P waves exceeds the number of QRS complexes.
-
PR intervals either lengthen (Mobitz I) or remain fixed until a sudden drop (Mobitz II).
-
The pauses are due to failed AV conduction, not premature atrial activity.
Enjoy this style of lecture and looking to learn more? Click below to learn more about how you can join my complete ECG course.
ECG With Reid Academy
Accredited by the AMA, AAPA, ANCC, ACPE & more.
