
Ever Seen Adenosine is Given in 2:1 Atrial Flutter? Here's What Happens...
Sep 28, 2025Adenosine is often used diagnostically and therapeutically in the emergency setting for supraventricular tachycardias (SVT). Its primary action is to transiently block conduction through the atrioventricular (AV) node, which terminates reentrant rhythms dependent on AV nodal conduction (e.g., AVNRT, AVRT).
But what if the rhythm is not an AV nodal reentry tachycardia, but atrial flutter with 2:1 conduction? The ECG response reveals both the anatomy of the atria and the functional role of the AV node.
Anatomy and Electrophysiology Refresher
-
Atrial flutter is caused by a macroreentrant circuit, most commonly within the right atrium around the cavotricuspid isthmus.
-
This circuit drives the atria at ~300 bpm.
-
The AV node acts as a gatekeeper, filtering impulses so the ventricles are not driven 1:1 at this dangerous rate.
-
In classic 2:1 conduction, every other atrial depolarization passes through the AV node, producing a ventricular response near 150 bpm.
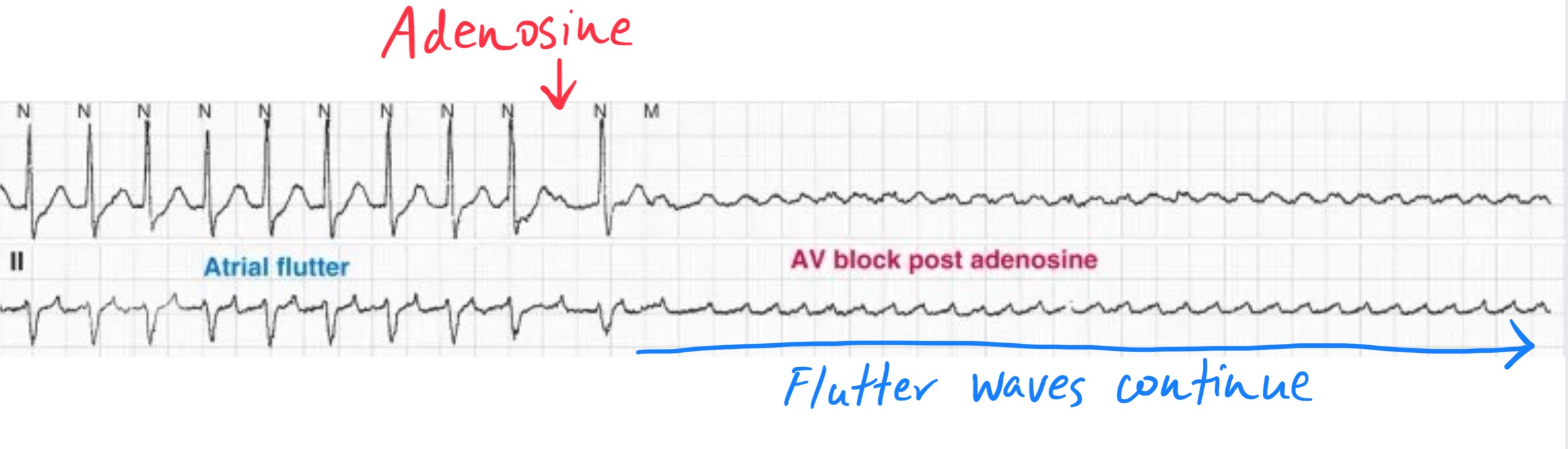
Adenosine does not stop the atrial reentrant circuit (since it’s not AV nodal–dependent). Instead, it temporarily blocks AV nodal conduction, unmasking the flutter waves.
ECG Findings After Adenosine in 2:1 Atrial Flutter
-
Immediate AV block
-
Adenosine transiently suppresses AV nodal conduction.
-
This often creates a brief period of complete AV block, during which flutter waves march through without ventricular response.
-
-
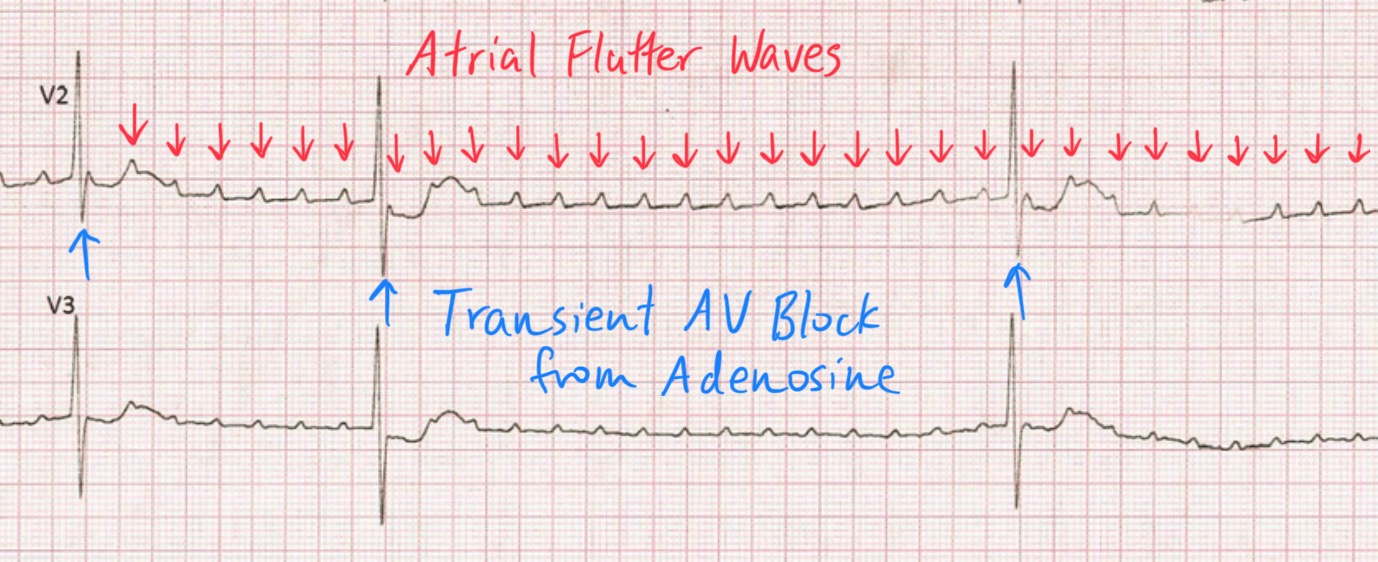
Unmasking of flutter waves
-
Without ventricular QRS complexes obscuring them, the classic “sawtooth” flutter waves become visible, especially in the inferior leads (II, III, aVF) and V1.
-
This allows the diagnosis of atrial flutter, which previously mimicked SVT with a narrow regular tachycardia.
-
-
Resumption of conduction
-
As the AV node recovers from the effect of adenosine, conduction resumes—often again at 2:1, with the ventricular rate returning to ~150 bpm.
-
In some cases, transient variable AV conduction (e.g., 3:1, 4:1) may appear before stabilization.
-
Why This Matters Clinically
-
SVT vs flutter distinction: Both can present as a narrow-complex tachycardia at 150–180 bpm. Adenosine unmasks atrial activity, distinguishing between AV nodal–dependent tachycardia (which terminates) and atrial flutter (which persists).
-
Anatomical insight: This demonstrates the AV node’s role as a filter. The atrial flutter circuit persists uninterrupted, but the AV node can be briefly silenced, exposing atrial activity.
-
Clinical pearl: A ventricular rate of ~150 bpm in a narrow tachycardia should raise suspicion for 2:1 atrial flutter. Adenosine is safe and useful diagnostically, but it will not terminate the arrhythmia.
Take-Home
When adenosine is given in 2:1 atrial flutter, the arrhythmia does not terminate. Instead, you see:
-
Transient AV block,
-
Exposure of classic sawtooth flutter waves,
-
Resumption of conduction once the drug wears off.
The key anatomical lesson is that the atrial flutter circuit is atrial-based, while adenosine only influences the AV node.
Enjoy this style of lecture and looking to learn more? Click below to learn more about how you can join my complete ECG course.
ECG With Reid Academy
Accredited by the AMA, AAPA, ANCC, ACPE & more.
