
Calculating AV Conduction Ratios in Atrial Flutter
Nov 27, 2025Atrial flutter produces one of the most organized patterns of supraventricular tachyarrhythmia, characterized by a rapid, regular atrial rate—typically around 300 beats per minute in classic cavotricuspid isthmus–dependent flutter. While the atrial activity is highly regular, the ventricular response is not determined by the atria alone. Instead, the anatomy and physiology of the AV node dictate how many of those atrial impulses actually reach the ventricles.
Understanding how the AV node filters atrial activity is essential for accurately calculating AV conduction ratios on the ECG and recognizing when the ventricular rate is physiologic versus dangerously rapid.
1. Atrial Flutter Cycle Length: Where the 300 bpm Comes From
Typical flutter involves a macroreentrant circuit around the right atrium, using the cavotricuspid isthmus (CTI) as part of the critical pathway. This circuit has a fixed conduction velocity and pathway length, producing a cycle length of roughly 200 ms (approx. 300 bpm).
This predictable atrial cycle is why flutter is the rhythm where AV conduction ratios are easiest—and most clinically important—to calculate.
2. The AV Node as the Gatekeeper: Anatomical Basis for Ratio Formation
While the atria may depolarize at 300 bpm, the ventricles cannot follow at that rate because of the structure and physiology of the AV node:
Dual AV Nodal Pathways (functionally)
-
Fast pathway: rapid conduction, long refractory period.
-
Slow pathway: slower conduction, shorter refractory period.
Although dual pathways are clinically most evident in AVNRT, the physiology still influences how the AV node handles rapid atrial input.
AV Node Refractoriness
The AV node has an absolute refractory period that is longer than the flutter cycle length.
This means not every flutter wave can propagate into the His–Purkinje system.
Thus, the node conducts in ratios:
-
2:1: every second flutter wave is transmitted
-
3:1, 4:1, 5:1, etc.
-
Variable conduction when refractoriness changes beat-to-beat
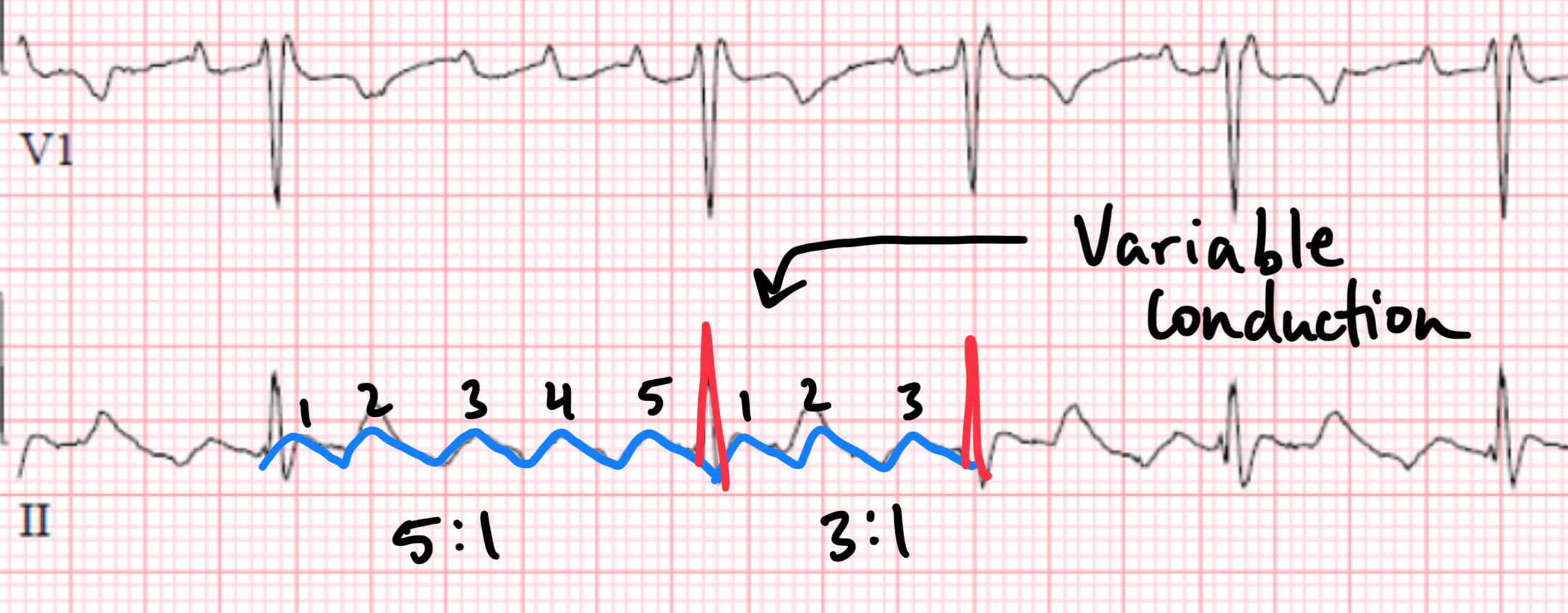
In essence, the conduction ratio is a direct readout of AV nodal refractoriness at any given moment.
3. How to Identify the Conduction Ratio on ECG (Rooted in Anatomy)
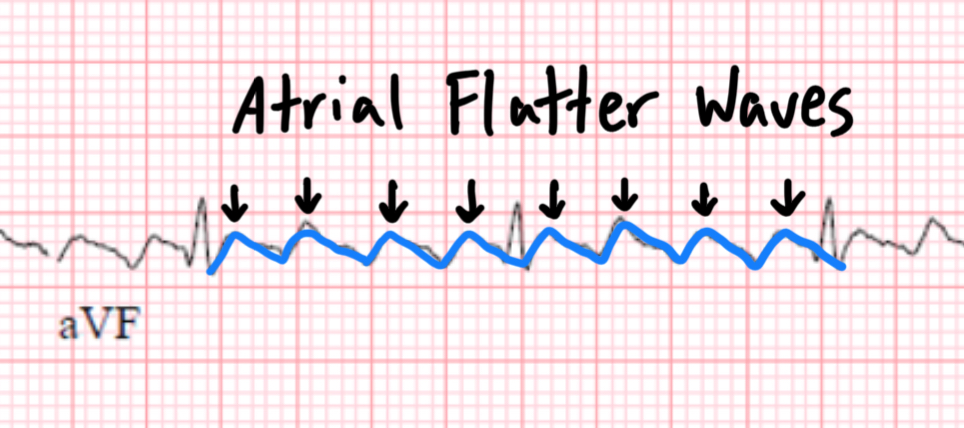
Step 1: Identify the flutter waves
Best seen in:
-
II, III, aVF (inferior leads)
-
V1
where the sawtooth pattern is most prominent.
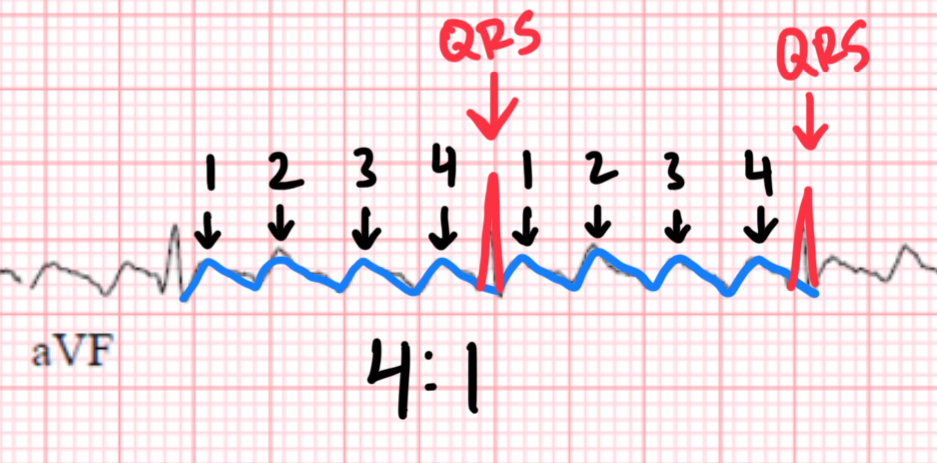
Step 2: Count atrial waves between QRS complexes
Because atrial flutter waves occur at a predictable cycle length (~200 ms), the ratio simply reflects how many of those impulses reach the AV node during its recovery window.
Examples:
-
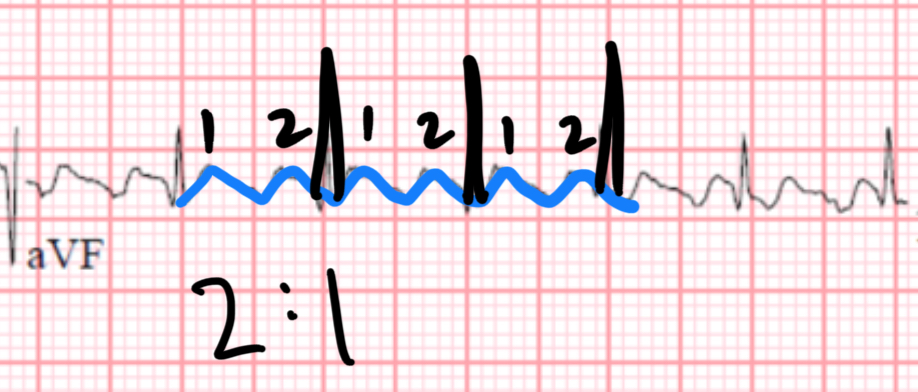
2:1 conduction
Atrial rate 300 → Ventricular rate ~150 bpm
One flutter wave conducts, the next hits the refractory node. -
3:1 conduction
Ventricular rate ~100 bpm -
4:1 conduction
Ventricular rate ~75 bpm
The consistent spacing of flutter waves reflects the anatomic reentry loop, while the ventricular response reflects AV nodal recovery dynamics.
4. Why the Ratio Changes: Autonomic and Structural Influences
Vagal tone
Increased parasympathetic activity prolongs AV nodal refractoriness, shifting conduction to higher ratios (e.g., 3:1 → 4:1 → 5:1).
Sympathetic stimulation
Shortens AV nodal refractory time, allowing faster conduction (higher ventricular rates).
Medications
-
Beta-blockers, calcium-channel blockers, digoxin: increase refractoriness → higher ratios
-
Sympathomimetics: decrease refractoriness → lower ratios
Intrinsic AV nodal disease
May force the ratio higher even in the absence of autonomic influences.
Accessory pathways
Importantly, atrial flutter with pre-excitation may produce dangerously rapid ventricular rates because accessory pathways lack decremental conduction.
This eliminates the normal AV nodal filtering mechanism.
5. Clinical Importance: The Ratio Isn’t Just a Number
Understanding the anatomy behind conduction ratios helps with:
-
Diagnosing flutter when the sawtooth pattern is subtle
(e.g., in 2:1 conduction where the atrial waves hide inside the QRS) -
Assessing hemodynamic stability
1:1 conduction (rare but possible) may produce ventricular rates approaching 300 bpm—an emergency. -
Guiding therapy
-
AV nodal blockers will increase the conduction ratio.
-
Enjoy this style of lecture and looking to learn more? Click below to learn more about how you can join my complete ECG course.
ECG With Reid Academy
Accredited by the AMA, AAPA, ANCC, ACPE & more.
